Abstract
This article applies recent recommendations by the US Institute of Medicine (IOM) that health professionals and researchers take a systems approach to improve health care quality. IOM identified four states of a systems approach as Identification, Description, Alteration and Implementation, that could be used to model components of healthcare to bring unified thinking to addressing areas where gaps may thwart optimizing patient care.
We applied the IOM approach to nonprescription drug-taking behavior, and for the first time describe a ‘Systems Cycle of Healthcare’ and its derivative, a ‘Systems Cycle of Self-care – OTC Medication-Taking Behavior’. The models are simple, intuitive, and appear useful in identifying gaps for governments and other organizations to target national and international initiatives to improve population-based responsible self-care.
We encourage other researchers and health professionals to expand this concept to other areas of self-care (e.g. lifestyle behavior change) and test our proposed model through rigorous research. We also believe the Systems Cycle of Self-Care will be useful for government, companies and professional schools in orienting advisory panels, employees and students who are new to the field of self-care.
Self-care is recognized as one of the four pillars of health care, the other three being primary, secondary and tertiary care1. Self-care has been defined as being ‘about people’s attitudes and lifestyle, as well as what they can do to take care of themselves when they have a health problem’2. This is a broad definition that includes individuals as independent consumers, patients under the care of a physician, and caretakers in charge of another person’s health (e.g., parent for a child). Self-care therefore encompasses a spectrum of activities that the individual would undertake independently, or in concert with support from practitioners, family and friends. These activities may include, for example: lifestyle choices (e.g., dietary regimens, physical activity, smoking, alcohol); medication-taking behavior; personal hygiene; and stress management. When an individual seeks or is offered support to manage their own health, the term ‘supported self-care’ is used, meaning actions by other individuals (e.g., healthcare professionals) to increase ‘people’s confidence and self-esteem, enabling them to take decisions about the sensible care of their health and avoiding triggering health problems.’1.
As a result, self-care spans all dimensions of healthcare, from the individual autonomously self-selecting an OTC medicine or dietary supplement, to the patient self-adhering to post-encounter action plans from primary, secondary and tertiary care practitioners; plans for which the patient is solely responsible prior to the follow-up visit. Whether independent or supported, the major theme emanating from the definition of self-care is that it must be patient-centered. Attitude, choice, personal decision-making, empowerment, and subsequent behavioral change are essential elements of self-care.
Because of its broad-reaching definition, self-care as a component of healthcare is a complex phenomenon. The U.S. institute of Medicine (IOM) acknowledges this complexity in its 1999, 2006 and 2013 calls for improvement in the quality of healthcare. In these reports, IOM described significant safety and cost-related gaps in healthcare3,4. Most recently, IOM concluded that: 20-30% of patients annually receive harm during hospital stays; 30% of healthcare expenditures are unnecessary or unneeded; improvement in the quality of care is stagnant due to the sheer complexity of medicine that strains human intelligence; and the poor interoperability of IT systems. Inconsistent use of scientific evidence results in 50% of U.S. patients not receiving care as recommended in accepted guidelines. Patient satisfaction is poor due to insufficient time being employed to explain their healthcare problems and share information, as well as less respect being accorded them than they feel is appropriate5.
Gaps in self-care in relation to Rx and OTC medication-taking behavior have also been documented independently6. For example, physicians typically spend less than one and a half minutes on medication counseling during an office visit, and in that time convey only 60% of essential medication information7,8. About 40-80% of information conveyed in a medical office visit is forgotten by the patient upon leaving the office9. In the retail pharmacy setting, 70% of those getting a prescription do not get counseling in the U.S., 50% of those getting a prescription medicine do not read or keep the detailed retail drug monograph stapled to, or inserted in, the dispensing bag, and about 60% of oral counseling information is forgotten after the pharmacist encounter10. With respect to consumers not under a physician’s care for a condition and selecting a nonprescription medicine for the first time, about 55% do not read the OTC Drug Facts label for active ingredients, while 66% report not referring to dosage information, and 80% to not reading the label for side effects11.
On this background, in July 2013 IOM once again called for a systems approach to healthcare interventions to define the elements and their interrelationships, and to model how they work individually and in assembly to effectuate patient care. With this type of approach, gaps in the scientific basis for the operational value of each element can be explored as a means to optimize and compare interventions in a more comprehensive way.
This paper draws on IOM’s approach to develop a simplified systems representation of the self-care component of healthcare and explores its application to consumer use of nonprescription medicines for self-care.
METHODOLOGIC CONSIDERATIONS:
IOM defines a systems approach to health as one that ‘applies scientific insights to understanding the elements that influence health outcomes, models the relationships between those elements; and alters design, processes, or policies based on the resultant knowledge in order to produce better health at lower cost.’5. IOM urges that all approaches ensure patient-centeredness as a central orientation.
Based on engineering approaches in other industries, IOM identified four general stages of the systems approach, as follows5:
1. Identification: ‘Identify the multiple elements involved in caring for patients and promoting the health of individuals and populations.’
2. Description: ‘Describe how those elements operate independently and interdependently.’
3. Alteration: ‘Change the design of organizations, processes, or policies to enhance the results of the interplay and engage in a continuous improvement process that promotes learning at all levels.’
4. Implementation: ‘Operationalize the integration of the new dynamics to facilitate the ways people, processes, facilities, equipment, and organizations all work together to achieve better care at lower cost.’
For the purposes of this paper, applying IOM’s general stages to medication-taking behavior for nonprescription medicines included: (a) ensuring each stage was represented in the final model; and (b) critically evaluating whether the order of the stages described by IOM would fit a simplified model or not. The first stage involved creating a list of elements in self-care with medicines, ranking the elements in terms of importance, and determining the sequence of the major elements. Ranking and sequencing were exercises that helped define interrelationships and interdependence of the basic system diagram of self-care. Ultimately, the model of the systems approach applied to OTC medication-taking was used to test the logic and practicality of the basic system approach to self-care.
Since patient-centeredness is a core component in IOM’s approach, and choice is fundamental to behavior change in self-care, the proposed model for medication-taking behavior was constructed to place the ultimate decision maker in a central position. In self-care this decision maker may be an individual under a physician’s supervision, a caretaker, or a consumer independently self-selecting and self-implementing self-care decisions.
RESULTS
Systems Cycle of Healthcare
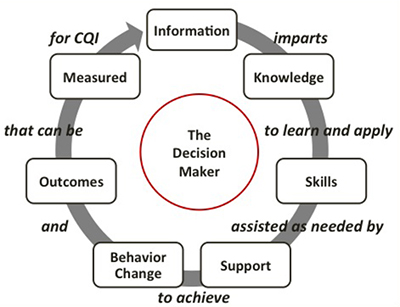
Figure 1 shows the seven stages of a proposed Systems Cycle of Healthcare comprised of the major elements of self-care. The core element is the ultimate decision maker who owns the system. The other major elements in sequence are: information; knowledge; skills; support; behavior change; outcomes; and measurement.
Information is placed as the initial element, since this relates to the foundational scientific database that is interpreted into knowledge. ‘Linkage elements’ are those that define the interrelationships between adjacent major elements. For example, ‘imparts’ is a verb linking information to knowledge.
Figure 1: Systems Cycle of Healthcare
 All rights reserved ‘Systems Cycle for Health Care’ sollerphd.com 2014
All rights reserved ‘Systems Cycle for Health Care’ sollerphd.com 2014
The relationship between elements and linkage elements (from Figure 1) can best be described as follows: credible scientific information imparts knowledge for the decision maker to learn and apply as skills to independently achieve the intended behavioral change. As needed, the decision maker may be supported by others or other information to be enabled to achieve that behavioral change. Behavioral change results in one or more outcomes that can be measured and evaluated for continuous quality improvement (CQI).
CQI is essential, since the informational foundation for the intended behavioral change may change over time. For example, drug approval may be based on efficacy studies. These studies are controlled explorations of the positive and negative effects of medicines in populations of a few thousand patients, who are defined by strict inclusion and exclusion criteria and follow narrowly defined protocols of drug administration. In the real world post drug approval, in-use effectiveness is generally defined in an ‘all-comer’ population, with broader inclusion criteria and less control over actual use of the medicine. With a greater denominator of use, it is more likely that rare side effects may be identified with use of a particular medicine. Thus, drug safety at time of approval does not necessarily capture all potential adverse effects associated with the drug’s use, and labeling information must be updated over time.
Systems Cycle of Self-Care – OTC Medication-Taking Behavior
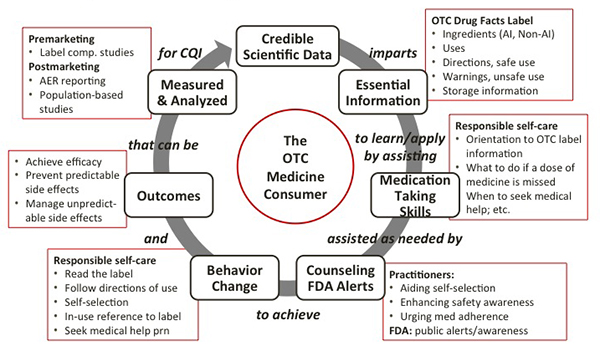
Application of the proposed Systems Cycle of Healthcare to over-the-counter (OTC) medication-taking behavior is shown in Figure 2.
Figure 2: Systems Cycle of Self-Care: OTC Medication-Taking Behavior
 All rights reserved ‘Systems Cycle of Self-Care – Example of OTC Medicine-Taking behavior’ sollerphd.com 2014
All rights reserved ‘Systems Cycle of Self-Care – Example of OTC Medicine-Taking behavior’ sollerphd.com 2014
Most notable is the central element, the OTC medicine consumer who is the ultimate decision-maker for most, if not all, nonprescription medication use. The OTC medicine consumer is defined here in two ways as an individual who is: (a) self-medicating or acting as a caretaker (e.g., parent), but not under the supervision of a physician for use of an OTC medicine which he or she has self-selected (e.g., for heartburn, headache, common cold etc.); (b) self-medicating or acting as a care-taker (e.g., parent) and under the supervision of a physician with a professional recommendation to use a specific OTC medicine.
The starting point is the Information element identified as access to a credible scientific database that helps define safe and effective use of the medicine. The information derives from self-selection, label comprehension and actual use studies as well as world-wide adverse experience reports and other published and non-published information. Detailed evaluation and discussion of criteria for safety and efficacy decisions that determine OTC marketing status in the U.S. has been recently published12,13.
Interpretation of the scientific basis of OTC availability derives the essential knowledge (i.e., directions for safe use and warnings against unsafe use, etc.) which is required for the OTC consumer to use the OTC product safely, and which is formatted in the US as the OTC Drug Facts label14. The OTC consumer is expected to learn and apply information in the Drug Facts label using medication-taking skills that enable self-selection of the product and safe and effective use. Without the OTC Drug Facts Label, the OTC product is considered not safe and effective for use.
Learning how to apply essential knowledge represents the acquisition of medication-taking skills. These skills include, for example, appropriate self-selection of the product based on its labeling, awareness of safe use directions on the label and certain general self-care practices (e.g., routine reading of medication labels when selecting and taking or administering an OTC medicine, following directions of use, asking questions if in doubt, retention of labeling during use for referral, adhering to dosage directions etc.). Medication-taking skills are the principal factor in determining the nature of the behavioral change directed by the OTC Drug Facts label. In this general example applied to all OTC medicines, the behavioral change is achievement of responsible self-medication, which can be summarized at a high level as: reading the label; taking as directed; asking questions of a provider if in doubt; and seeking medical help in case of an serious emergent side effect.
Medication-taking behavior, to a greater or lesser extent, leads to an outcome that is intended, uncertain or not intended. Under a scenario that the medication was selected for the right condition, by a consumer who follows directions of use in terms of the right dose at the right interval, and heeds warnings against unsafe use including seeking immediate medical help as needed, the user should achieve the intended outcome. This outcome is defined as a consumer experience of responsible self-care in which there is the expected level of effectiveness, a lack of predictable side effects, and reasonable management of unpredictable side effects (e.g., drug allergy) as early in their course as possible. While the foregoing scenario depicts optimal benefit from an OTC medicine, risk is inherent in this model based on the degree to which the consumer undertakes responsible self-care and the probability of drug-induced adverse outcomes from less than optimal self-care.
Virtually all outcomes can be measured, some more easily and at a more reasonable cost than others. In the U.S., many Rx-to-OTC switch products are tested prior to approval for: the ability of consumers, even those with low health literacy, to appropriately self-select and comprehend the label; and use of the product label in ‘actual use’ settings12,13. In some cases elements of labeling also are reviewed and evaluated post-marketing15. Mainly however, measurement of outcomes from consumer behavior with OTC medicines is by means of required adverse experience reporting to the FDA, including spontaneous reports from consumers, practitioners and lawyers to either companies or FDA, as well as through new information from peer-reviewed publications in the medical literature. The actual use of the OTC Drug Facts label is rarely studied post-marketing, and usually only in relation to surveys on retrospective self-reported use of the OTC drug label6,12,16. Nonetheless, as new information arises and is deemed essential for safe and effective use of OTC medicines, OTC labels are revised representing a CQI process of information enhancement. Notable recent examples of post-marketing changes to OTC Drug Facts labels include the liver damage and stomach bleeding warnings for OTC acetaminophen and OTC aspirin respectively, cardiovascular warnings for OTC NSAIDS and improvement of the drug allergy alert for acetaminophen17,18.
DISCUSSION
The Systems Cycle for Self-Care as it pertains to medication-taking behavior represents a useful framework for examining risk management approaches to medication use, addressing gaps in self-care relating to OTC medication-taking behavior, and evaluating approaches to education of the public on responsible self-care.
Past Approaches to Systemizing Risk Management by the FDA
Through the emphasis by IOM on patient-centeredness in approaches to systems-based innovations, the Systems Cycle of Self-Care demonstrates the value of adding granularity to diagrams of standard risk management systems19. In May 1999, the FDA Task Force on Risk Management issued a report to the FDA Commissioner calling for a systems approach to risk management by the agency. The Task Force concluded that the basic processes that are advocated at the Federal level to manage risk are those that FDA uses: assessment (estimation and evaluation of risk; confrontation (determining acceptable level of risk in a larger context); intervention (risk control action); communication (interactive process of exchanging risk information) and management evaluation (measure and ensure effectiveness of risk management efforts). Yet, if FDA’s risk management approach is actually defined by the conceptual approaches shown in FDA’s modeling (shown in Figures 3 and 4), then the diagrams represent more of a defense to external negative commentary. While Figure 3 identifies the generally accepted process of drug development, Figure 4 speaks to how FDA manages all its stakeholders. Yet, today IOM urges patient centeredness and the Cycle of Self-Care adopts that concept by identifying the core element as the consumer – the ultimate decision maker when it comes to, for example, using OTC medicines for self-limiting conditions or taking Rx medicines to treat chronic conditions. We urge government agencies to update their risk management approach to apply the Systems Model of Self-Care as a basic model for considering medication-taking behavior.
Figure 3
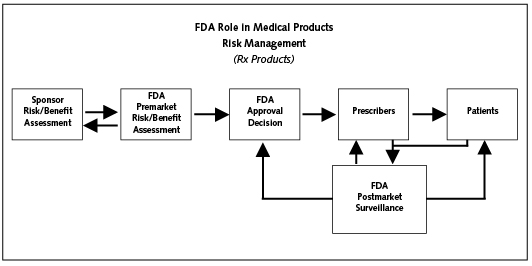 From: Food and Drug Administration Task Force on Risk Management. Managing the Risk from Medical
From: Food and Drug Administration Task Force on Risk Management. Managing the Risk from Medical
Product Use: Creating a Risk Management Framework. Report to the FDA Commissioner. May 1999.
Figure 4
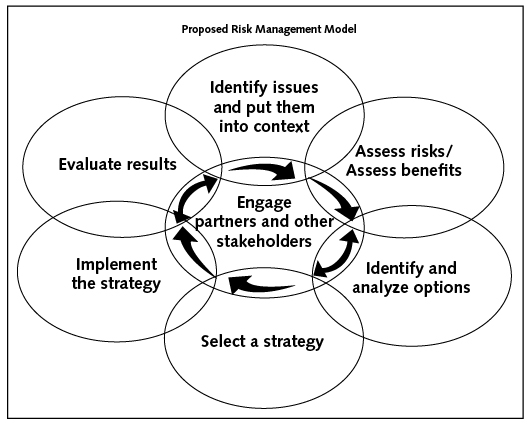 From: Food and Drug Administration Task Force on Risk Management. Managing the Risk from Medical
From: Food and Drug Administration Task Force on Risk Management. Managing the Risk from Medical
Product Use: Creating a Risk Management Framework. Report to the FDA Commissioner. May 1999.
Educating the Public
The Food and Drug Administration and the National Council for Patient Information and Education (NCPIE) have recently introduced OTC medication education programs to help consumers as well as children gain an understanding of the OTC Drug Facts label and medication-taking skills (e.g., read the label for ingredient content, and avoid taking two medicines with the same active ingredient).
Medicines in My Home (MIMH) is a multimedia FDA-initiated educational program to teach consumers from adolescence through adulthood how to choose over-the-counter medicines and use them safely20. MIMH is presented as a Web education program on CDERLean and as an online resource in the form of ‘Rooms’ which contain presentations, print materials, and resources that teachers, students and adults can use online or download. On May 8, 2014, NCPIE partnered with a large pharmaceutical firm to extend this concept nationwide through stakeholder adoption of research-based education program entitled ‘OTC Literacy.’21. Young adolescents or ‘tweens’ begin to self-administer medicine around 11 years old, or around 5th or 6th grades in the U.S.22. The OTC Literacy program was launched in 2013 in schools nationwide, using informational resources and engaging educational activities designed for parents and teachers of tweens to increase knowledge of OTC safety and responsible use.
In the May 8th meeting, the Systems Cycle of Self-Care was used to orient new stakeholders of the OTC Literacy program as a foundation for understanding self-care and medication-taking behavior, as well as to emphasize the importance of tracking and continuous quality improvement to ensure sustainability. We encourage this type of effort internationally, and development of inter-country collaboration on best practices in helping to raise awareness and skills acquisition in consumers from young adolescents to older adults.
Applying the Systems Cycle of Self-Care to Gaps Analysis
As noted in the systems diagram (Figure 2), medication-taking behavior can be segmented into its elemental steps and interlinking relationships. The value of diagrammatically representing the Systems Cycle of Self-Care in a tangible model allows core questions to be asked about what we know and do not know about consumer behavior and responsible self-care.
While in some countries research on consumer behavior is required to support approval of most Rx-to-OTC switch products, as noted above, relatively little is known about broader population-based behavior post-marketing, and trends over time. With self-care as one of the pillars of healthcare, it is important that we measure the impact of self-care behaviors on health outcomes. It is also important to know how consumers of OTC medicines can best be informed when new information e.g. on adverse events, emerges. Unless we are confident in how consumers will behave in response to changing information, it is difficult to be sure that a positive benefit to risk equation for a particular OTC drug can be maintained.
Further, little is also known about how young people will respond to educational programs on responsible self-care and if such programs have a longer term impact on, for example, medication adherence. We also need to establish the best tools and approaches to teaching older consumers, and those whose medical condition may suddenly require them to think more seriously about both disease and medication management. These are just a few examples of the types of questions that naturally flow from a creative view of the System Cycle of Self-Care. This approach could lead to a clearer definition of the public health goals of self-care, better study of population-based outcomes, and development of a framework for tracking outcomes for quality improvement efforts. We encourage an international dialogue on this issue.
CONCLUSION
We have shown that the application of principles set forth by the U.S. Institute of Medicine for a systems approach to healthcare to nonprescription medication-taking behavior by consumer is feasible, and appears to be a useful tool to identify gaps in the system with an eye to national and international efforts to promote responsible self-care by large populations of consumers. In our view, our modeling approach can be adapted to other systems and subsystems of self-care. We encourage national and international efforts to take up this issue as exemplified by new efforts of NCPIE, FDA and associated stakeholders.
Correspondence to: RW Soller PhD, Principal, sollerphd.com, Houston, TX, USA. Email sollerrw@pharmacy.ucsf.edu or rwsoller@gmail.com.
References
- National Health Service. Supporting Self Care. Updated 2011.
Reference Link - Chambers R, Wakley G, Blenkinsopp A. Supporting Self-care in Primary Care. 2006. Radcliffe Publishing Ltd. Oxon, UK.
- Institute of Medicine. To Err I s Human: Building a Safety Health Care System. November 1999.
Reference Link - Institute of Medicine. Precventing Medication Errors. July 2006.
Reference Link - Institute of Medicine. Bringing a Systems Approach to Health. July 10, 2013.
Reference Link - Soller RW, Shaheen C. Self-reported Consumer Medication Taking Behavior in the United States: Evidence for a Medication Education Gap. SelfCare 2011;2(3):66-75.
- Tarn DM, Paterniti DA, Kravitz RL, Heritage J, Liu H, Kim S, Wenger NS. How much time does it take to prescribe a new medication? Patient Educ Couns. 2008;72:311-319.
- Tarn DM, Heritage J, Paterniti DA, Hays RD, Kravitz RL, Wenger NS. Physician communication when prescribing new medication. Arch InternMed 2006;166(17):1855-1862.
- McGuire LC. Remembering what the doctor said: organization and adults’ memory for medical information. Exp Aging Res. 196;Oct-Dec(4):403-28.
- Feifer, RA, Greenberg L, Rosenberg-Brandl S, Franzblau-Isaac E. Pharmacist Counseling at the Start of Therapy: Patient Receptivity to Offers of In-Person and Subsequent Telephonic Clinical Support. Popul Health Manage 2010.13(4);189-193.
- Harris Interactive. Uses and attitudes about taking over-the-counter medicines. [Internet] Rockville (MD): National Council on Patient Information and Education; 2003. [cited 2011 Apr 15].
Reference Link - Soller RW, Chan P, Shaheen C. OTC Considerations for Expanding Access to Nonprescription Medicines: A Critical Synthesis of Questions from FDA to its Advisory Committees on Rx-to-Switch. SelfCare 2011;2(5):117-138.
- Soller RW, Shaheen C. The Switch Considerations List: 'Considerations for Rx-to-OTC Switch' Refined by a Critical Synthesis of FDA Comments on Expanded Access for Naloxone. SelfCare 2012;3(6):121-137.
- U.S. Code of Federal Regulations: 21 CFR Sec. 201.66 Format and content requirements for over-the-counter (OTC) drug product labeling.
Reference Link - Soller RW, Shaheen D, Yen J, Rose J, Lightwood C. Label Comprehension Studies Supporting a Revised Drug Allergy Alert for Nonprescription NSAIDs. Therapeutic Innovation and Research Journal (formerly, Drug Information Journal) 2012;46(3):336-343.
- Harris Interactive. Uses and attitudes about taking over-the-counter medicines. [Internet] Rockville (MD): National Council on Patient Information and Education; 2003. [cited 2011 Apr 15].
Reference Link - Food and Drug Administration. COX-2 Selective (includes Bextra, Celebrex, and Vioxx) and Non-Selective Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). April 7, 2005.
Reference Link - Food and Drug Administration. FDA Drug Safety Communication: FDA warns of rare but serious skin reactions with the pain reliever/fever reducer acetaminophen. August 1, 2013.
Reference Link - Food and Drug Administration Task Force on Risk Management. Managing the Risk from Medical Product Use: Creating a Risk Management Framework. Report to the FDA Commissioner. May 1999.
- Food and Drug Administration. Medicines in My Home (MIMH).
Reference Link - National Council of Patient Information and Education. Promoting OTC Literacy –Beyond the Classroom. May 8, 2014.
Reference Link - American Association of Poison Control Centers. The American Association of Poison Control Centers and Scholastic Expand Collaboration to Educate Tweens on Over-the-Counter Medicine Safety. November 4, 2013.
Reference Link