Abstract
BACKGROUND:
Irritant diaper dermatitis (IDD), also called Napkin Dermatitis or Nappy Rash, is the most common dermatosis of the diaper area, resulting from prolonged contact of the skin with urine and faeces. The skin of young infants (<12 months) is structurally and functionally immature, exhibiting increased permeability to water, irritants and allergens, and elevated pH. These features make young infant skin particularly pre-disposed to IDD. Following improvements in diaper care, IDD management has now focussed towards prevention. However, traditional barrier treatments have been often less than ideal for repeated application to the immature, fragile skin of young infants. An IDD expert panel recently reached a consensus on nine standards for an ideal IDD preparation, highlighting the need for clinical testing in infants and the inclusion of only components with demonstrated safety and efficacy. Consequently, a new IDD formulation, Bepanthen Extra Protection was designed as a preventative IDD preparation for use in young infants.
OBJECTIVE:
To describe Bepanthen Extra Protection, report clinical safety and efficacy data, and outline how it adheres to the nine standards of an ideal IDD preparation.
RESULTS:
In vitro tests demonstrate that Bepanthen Extra Protection has anti-urease activity, is water resistant, and has anti-friction properties similar to zinc oxide (ZnO) lipophilic paste. In clinical studies in adults it was shown to be non-irritant and non-sensitising. It is perfume free, contains no anti-septic ingredient, is convenient to use and due to its transparent layer the skin status is easy to assess without need for removal. Furthermore, in infant studies Bepanthen Extra Protection was equivalent to ZnO lipophilic paste in both protecting and soothing infants who were predisposed to IDD.
CONCLUSION:
Bepanthen Extra Protection is well-tolerated, free from perfumes and anti-septics, convenient to use, and is an effective preparation for the prevention and treatment of IDD, in infants (≥3 months).
INTRODUCTION
Irritant diaper dermatitis (IDD) is a form of contact dermatitis and is the most common inflammatory dermatitis of the gluteal (diaper) area. IDD typically presents in infants between 3 weeks and 2 years of age, with a peak onset at 3–12 weeks and peak prevalence at 9–12 months1,2. Increasing prevalence of IDD can be correlated to an increase in the volume of urine and faeces, with more severe IDD occurring in younger infants who have a greater number of bowel movements per day2,3. IDD is very common amongst infants during their first year of life, with approximately 50% experiencing a mild form of IDD, 20% experiencing a moderate form, and 5% presenting with the most severe form of the condition2,4. IDD is a multi-factorial disease and occurs as a result of several irritants interacting with one another at the skin’s surface1. Prolonged contact and interaction of urine and faeces with the skin is the most important factor in the pathology of IDD. Several mechanisms contribute to the development of IDD, including maceration (prolonged wetness), increased alkalinity, activation of faecal digestive enzymes and friction1,5.
The skin of young infants (3–12 months), is structurally and functionally different to that of older infants (>12 months), and these differences can predispose them to IDD6. In particular, the network of microrelief lines is denser in the stratum corneum (SC) of young infants than in older infants. Consequently, young infants have a larger surface area-to-volume ratio at the skin surface which, in turn, increases the level of absorption by the skin, leading to maceration and the potential accumulation of allergens/sensitisers in the epidermis6. A thinner layer of collagen bundles beneath young infant skin, coupled with an SC and an epidermis that are 30% and 20% thinner than in older infants, respectively, leaves the skin more vulnerable to environmental damage6. By comparison with the skin of older infants, the skin of younger infants is still maturing and unable to regulate its water balance7. Transepidermal water loss (TEWL) and water content are higher in the skin of younger infants, which is therefore more susceptible to skin damage (maceration and/or dehydration) than in older infants7. Overall, these features suggest that, due to its immature and fragile nature, young infant skin requires extra care during the first months of life in comparison to older infant skin.
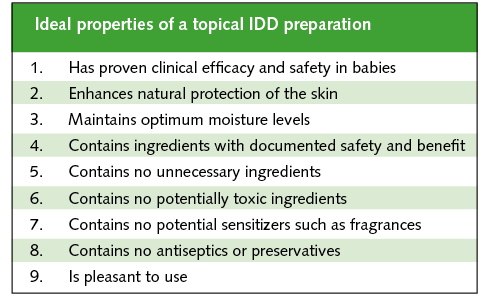
Given the significant differences in the skin of young infants (<12 months), the ideal composition of a topical IDD treatment has yet to be determined or developed. In June 2012, an international expert panel of dermatologists and paediatricians convened in London to discuss the optimal management of IDD (an update of a previous meeting held in 2003)8. The panel reviewed and reached consensus on the standards for the ideal topical formulation for IDD, increasing the previous seven standards and/or key properties to a total of nine (Table 1)9. The panel also agreed that, despite a relatively high incidence of IDD, improvements in diapers and wipes, and better standards of skin care, have now altered the focus of IDD management from a treatment to a preventive approach requiring careful attention to the formulation of barrier ointments1,9. The aim of this article is to describe Bepanthen Extra Protection, report data which evaluated its efficacy and safety profile, and address how the formulation adheres to the nine standards outlined above, as well as highlighting the importance of preventing IDD, particularly in younger infants (<12 months).
Table 1. The nine standards of an ideal IDD preparation.
BEPANTHEN EXTRA PROTECTION
A new Bepanthen preparation (Bepanthen Extra Protection) has been developed to protect and treat infant skin in the diaper area. It is a convenient to use water-in-oil ointment containing vitamins, lipids and humectants and is free from perfumes, known hyperallergenic and anti-septic ingredients. It forms a non-occlusive and transparent protective layer which allows easy assessment of the skin status underneath without the need for removal. The new formulation has been developed for protection against IDD, and can be regularly applied to young infants’ skin. Key ingredients in the new formulation include vitamin B3, which has anti-urease activity and promotes the synthesis of key skin lipids (ceramides, cholesterol and free fatty acids)10,11; panthenol (provitamin B5), which moisturises the skin and stabilises the skin barrier; phospholipids, which act to replace lost natural lipids12-14; and emollients (e.g. meadowfoam seed oil) which moisturise the skin and reduce friction at the skin’s surface. These components act in concert to prevent IDD by regulating skin hydration, preventing maceration, reducing friction, helping to maintain pH, and decreasing activation of faecal digestive enzymes (ureases).
IN-VITRO STUDIES
Bepanthen Extra Protection was assessed for its chemical, physical and biological properties, in both in vitro and clinical settings. Studies were conducted to determine the physical ability of the Bepanthen Extra Protection preparation to be water resistant and to retain water. Water resistance was measured by placing known amounts of Bepanthen Extra Protection and zinc oxide (ZnO) lipophilic paste into an aqueous medium for 1 h at 37°C under agitation. The samples were dried and re-weighed, with the loss in weight of each preparation an indication of its water resistance. Bepanthen Extra Protection and ZnO lipophilic paste were very water resistant, both exhibiting <2% change in mean weight loss (Table 2).
Water retention was studied using a methodology adapted from the European Standard BS EN 13726-2 for vapour transmission15. Briefly, standard amounts/depths of Bepanthen Extra Protection and Vaseline (petrolatum) were added to a mesh covering a collagen film. Transmission of de-ionised water through the preparations was measured after 24h, at 37°C and ≤20% humidity. The mean moisture vapour transmission rate (MVTR) of Bepanthen Extra Protection was higher than Vaseline, demonstrating that Bepanthen Extra Protection is not completely occlusive (Table 2).
Table 2. In vitro characterisation of the physical and biological properties of Bepanthen Extra Protection.
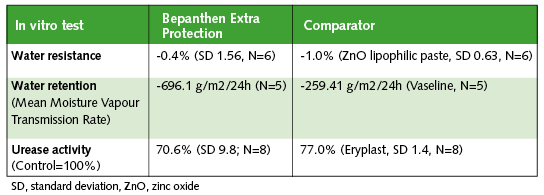
Since pH changes to the skin are usually as a result of hydrolysis of urea to ammonia and carbon dioxide by faecal ureases, the effects of Bepanthen Extra Protection, a comparator or placebo on urease activity were subsequently tested. Bepanthen Extra Protection, the comparator or placebo were incubated with known amounts of urea and urease. The quantity of ammonia (which correlates to urease activity) was detected by ultraviolet (UV) measurement following a colorimetric reaction with indophenol (Berthelot reaction)16. Ammonia generation and therefore urease activity was inhibited by 29.4% and 23.0% compared to control in the presence of Bepanthen Extra Protection and the comparator, respectively, although this difference was not significant (Table 2).
The anti-friction properties of the Bepanthen Extra Protection formulation were also assessed. Changes in viscosity of Bepanthen Extra Protection and the comparator product, ZnO lipophilic paste, were examined under shear stress (an indirect measurement of friction). Each formulation was placed in a rheometer under increasing pressure and rotation (sheer stress), at both room temperature and 37°C, for 5 min17. As sheer stress increased, both preparations demonstrated similar decreases in viscosity (i.e. decreases in friction) at both room temperature and 37°C; however, only Bepanthen Extra Protection demonstrated a delayed recovery of viscosity following removal of shear stress (thixotropy), at 37°C (Figure 1 and Figure 2). A decreased viscosity under shear stress, and a positive thixotropic profile, as for Bepanthen Extra Protection, are indicative of good anti-friction properties.
Figure 1. Shear-thinning profile of Bepanthen Extra Protection at 37oC for 5 minutes.

Figure 2. Shear-thinning profile of zinc oxide ointment at 37oC for 5 minutes.

TOLERABILITY IN ADULTS
The tolerability of the Bepanthen Extra Protection preparation was first tested in an adult population. Patch testing of the forearms conducted in 20 healthy adult volunteers (21–65 years) did not result in any skin abnormalities following macroscopic examination at 30 mins and 24h post application with both a Mean Irritation Index of 0, indicating that it is non-irritant (data not shown).
A more extensive open and intra-individual tolerability study of 21 adults (19–58 years) with sensitive skin was conducted over 21 days (Bepanthen Extra Protection applied twice daily). No clinical features of skin irritation (erythema, oedema, dryness, desquamation, roughness or vesicles) were reported by physicians during this study (data not shown). The Bepanthen Extra Protection preparation was also tested for its sensitising potential: 100 adults with normal skin were sensitised using the method of Marzulli and Maibach (1974)18. Skin was exposed for 3 weeks (Bepanthen Extra Protection applied three times per week), followed by a 2-week non-treatment period. Clinical evaluation was conducted following Bepanthen Extra Protection challenge on days 38 and 40 (week 6). No skin reactions were reported either during the sensitisation phase or following Bepanthen Extra Protection challenge on days 38 and 40, indicating that it is non-sensitising and non-irritating in adults (data not shown).
IDD STUDIES IN INFANTS (3−24 MONTHS)
Following successful testing in adults, Bepanthen Extra Protection was assessed in two studies in infants (3–24 months) to determine its ability to prevent and treat IDD. Both studies were double-blinded, randomised, comparator-controlled (ZnO lipophilic paste), parallel group studies, and conducted under paediatric control. ZnO lipohilic past was used as comparator because of its widespread use in IDD and because asking parents to not use any product at all either for prevention or treatment, was not seen as ethically justified. The studies were conducted according to the Helsinki Declaration on Ethical Principles for Medical Research Involving Human Subjects (1964), and were also approved by local ethics committees19. For inclusion in the study, infants had to be healthy, aged 3–24 months, have skin phototype I−III according to the Fitzpatrick scale20; and parental consent had to be provided. Infants were excluded if they: exhibited signs of cutaneous pathology on the studied zones (e.g. eczema); had received topical or systemic treatment liable to interfere with study products in the 4-weeks prior to enrolment; were enrolled in another clinical/cosmetic trial; or if they no longer used diapers.
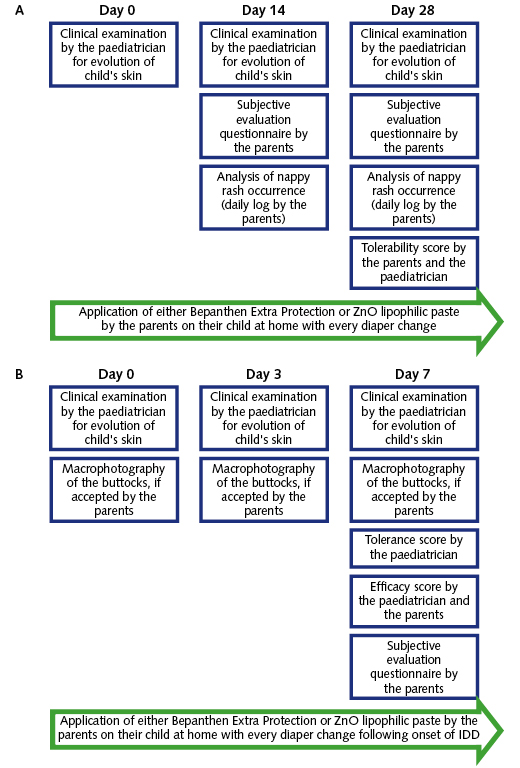
The prevention trial was conducted over the course of 28 days. In total, 109 infants were enrolled into the study and received topical treatment (n=55 Bepanthen Extra Protection and n=54 ZnO lipophilic paste) at each diaper change. Global tolerance scores were recorded at days 14 and 28, and determined from a combination of clinical (intensity/extent of erythema, vesicles, oedema, dryness, desquamation, roughness and others) and parental (erythema, anxiety/crying, scratching, warm sensation and others) observations based on a four-point scoring system (Figure 3A).
Figure 3. Protocol for (A) prevention and (B) treatment studies in infants (3–24 months)
Bepanthen Extra Protection was found to be well tolerated at the cutaneous level with tolerability scores from both paediatricians and parents reported as predominantly ‘very good’ or ‘good’ (Figure 4A). Overall, almost 70% of infants did not experience a single incidence of erythema with either Bepanthen Extra Protection (69.8%) or ZnO lipophilic paste (69.2%) during the 28-day study, as rated daily by parents. The observed erythema was rated as light and not persistent in the majority of patients (26.6% for Bepanthen Extra Protection and 27.1% for ZnO lipophilic paste) (Figure 4B). This is in line with the paediatricians’ assessment, observing only slight erythema in some cases with each preparation at days 14 and 28, which was considered to be clinically insignificant as it did not lead to the development of IDD. This demonstrates the prevention of the occurrence of (clinically relevant) diaper rash in the majority of subjects (about 96% both for Bepanthen Extra Protection and the ZnO lipophilic paste).
Figure 4A. Global tolerability (determined by parents and paediatricians) of Bepanthen Extra Protection following 28 days of treatment in infants.

Figure 4B. Daily rating of erythema during 28 days of treatment in infants with Bepanthen Extra Protection (determined by parents).

Furthermore, in comparison with the buttocks’ initial state, neither preparation induced any significant change in parent-assessed functional score (erythema, anxiety/crying, scratching or warm sensation; data not shown) suggesting that Bepanthen Extra Protection and ZnO lipophilic paste are equipotent in their ability to prevent IDD. According to subjective parental evaluations, Bepanthen Extra Protection was appreciated for its properties and efficacy after 28 days; in particular its ability to protect infant skin and prevent IDD onset (96%), as well as ease of use (100%) (Table 3).
Table 3. Parents’ subjective evaluation questionnaire for Bepanthen Extra Protection in infant prevention and treatment studies.

The treatment trial was conducted in 50 infants, who were randomised to receive Bepanthen Extra Protection (n=25) or ZnO lipophilic paste (n=25) for 7 days after the first appearance of erythema (Figure 3B). Global efficacy scores were recorded at days 3 and 7, from a combination of clinical (intensity/extent of erythema, vesicles, oedema, dryness, desquamation and roughness) and parental (erythema, anxiety/crying, scratching and warm sensation) parameters. Standardised macrophotography was also used to document changes in erythema at days 0, 3 and 7. Bepanthen Extra Protection was well tolerated at the cutaneous level, having efficacy scores from paediatricians and parents reported as predominantly ‘very good’ or ‘good’ (Figure 4C). Bepanthen Extra Protection and ZnO lipophilic paste exhibited similar activity, decreasing both the intensity of erythema and extent of IDD in infants (≥3 months) over a 7-day period (Figure 5). Similarly to the prevention trial, parental subjective evaluations confirmed that Bepanthen Extra Protection was appreciated for its properties and efficacy, with all parents (100%) agreeing that it protects and moisturises infant skin, reduces redness, is adapted for a child’s sensitive skin, and is easy to use (Table 3).
Overall, Bepanthen Extra Protection, a convenient to use water in oil formula, was shown to successfully prevent and treat IDD in infants as young as 3 months, and its efficacy and tolerability were similar to ZnO lipophilic paste.
Figure 4C. Global efficacy (determined by parents and paediatricians) for Bepanthen Extra Protection after 7 days of treatment following first signs of IDD in infants.

Figure 5. Changes in scores of extent of IDD over 7 days of treatment.

DISCUSSION
The skin of young infants (<12 months) is immature compared to that of older infants, with stratum corneum being up to 30% and epidermis up to 20% thinner, exhibiting increased absorption and TEWL, and elevated pH1,6. Consequently, the immature skin of young infants, coupled with an increased frequency of bowel movements/stools and urinary incontinence in their first months, has an increased risk of developing IDD3,8. Recently, the IDD management paradigm has moved towards prevention, supported by improvements in infant skin care and advances in diapers and wipes. However, there is a paucity of publications addressing IDD prevention, and currently available IDD preparations do not adequately address the need for repeated daily application and the fragile nature of young infant skin9. The new Bepanthen Extra Protection formulation was subsequently developed to proactively prevent the onset of IDD, by maintaining and enhancing skin barrier integrity, whilst being safe for repeated daily application in infants as young as 3 months following expert recommendation outlining 9 standards of an ideal IDD barrier preparation (Table 1).
Meeting the first standard, the clinical efficacy and safety of Bepanthen Extra Protection was shown in several studies. Skin sensitisation studies and tests on sensitive skin in adults demonstrated that Bepanthen Extra Protection is non-sensitising and non-irritant in nature. Studies of the preparation have demonstrated its ability to prevent and treat IDD in infants as young as 3 months. Bepanthen Extra Protection was shown to be well tolerated and effective in preventing the development of IDD over 28 days in infants between 3 and 24 months. Furthermore, it prevented the occurrence of any erythema and roughness in 70% of all infants during 28 days of treatment with only slight, transient erythema in another 26%, and was demonstrated to have similar activity to ZnO lipophilic paste. This was used as comparator due its very wide spread use in IDD despite being less convenient for daily application as a paste in a preventive setting and not allowing a good assessment of the skin status underneath. In the cases where a slight erythema could be observed these were rated as not clinically relevant and did not lead to the development of IDD. Parents appreciated Bepanthen Extra Protection’s properties and efficacy; in particular its ability to protect infant skin and prevent IDD onset. In a 7-day treatment trial, Bepanthen Extra Protection decreased the intensity and extent of IDD in young infants, and again was as effective as ZnO lipophilic paste. As it was not seen as ethical to compare to an untreated control group, asking parents to not use any product at all, as earlier studies indicate the positive effects of a preventive use of barrier preparations21, it is not possible to compare the effects directly to no intervention. Despite this limitation the two studies demonstrate that the new formulation provided a barrier across the skin as effective as a lipophilic paste, but was considered easy and pleasant to use by parents, without the need for removal between diaper changes, thereby improving the likelihood of compliance especially in a preventive setting.
Bepanthen Extra Protection, in contrast to the comparator, contains a number of key components which act to maintain skin barrier integrity by promoting hydration, reducing mechanical and biochemical damage, and protecting and repairing the skin barrier to match standards 2 and 3 (Table 1). Provitamin B5 (panthenol), an effective moisturiser, maintains hydration and protects infant skin from mechanical damage12,14,22. Panthenol is also known to support the skin’s regeneration processes, thereby stabilising the skin barrier12,14. Skin hydration is also maintained by the inclusion of natural lipids and oils (e.g. meadowfoam seed oil). These lipids replace lost natural lipids, thereby stabilising and repairing the skin barrier23-26. Bepanthen Extra Protection also contains vitamin B3, which has significant anti-urease activity, and acts to prevent a rise in pH by inhibiting the deamination of urea to ammonia10. Furthermore, vitamin B3 in combination with Bepanthen Extra Protection’s pH neutral formulation helps to prevent the activation of faecal enzymes (which work in alkaline milieu), which can cause irritation and damage to the skin barrier1,27. The Bepanthen Extra Protection formulation forms a transparent ‘breathable’ waterproof layer on the skin that allows normal TEWL to occur, and prevents maceration and occlusion of the SC, processes which can block skin repair mechanisms and raise pH, leading to skin barrier damage8. Finally, the anti-friction formula of Bepanthen Extra Protection has strong lubricating properties consisting of a water-in-oil emulsion rich in lanolin and vegetable oils, which help to prevent mechanical damage to young infant’s skin.
Bepanthen Extra Protection contains only ingredients with documented safety and benefit as outlined in the standards 4 to 8 (Table 1). Agents such as anti-bacterials and antiseptics, which do not ameliorate IDD and can disrupt the commensal skin flora promoting opportunistic secondary infections, were not included in the Bepanthen Extra Protection formulation in contrast to the comparator product which contained benzyl alcohol1,5,8. Furthermore, compounds such as ZnO that have traditionally been added to IDD preparations were not considered due to a lack of published controlled studies supporting their benefits in ameliorating infant IDD28. Preservatives and fragrances which have no clinical benefit in preventing or treating IDD, and which can induce allergic reactions, were also excluded from the preparation whereas the comparator contained three of the 26 ingredients with known sensitizing potential and to be labelled in cosmetics in the European Union (benzyl alcohol, benzyl cinnamate, benzyl benzoate)29.
Finally, Bepanthen Extra Protection meets the 9th standard by being a convenient to use water in oil formulation leaving only a transparent layer on the skin making it easy to assess the skin status of the infant’s buttock skin without the need for removal of the product.
In conclusion, young infant (<12 months) skin is immature compared to older infants, and as such requires extra protection from the causes of IDD. However, current preparations have not been optimised for the prevention of IDD in these young infants. Bepanthen Extra Protection has been developed adhering to the nine consensus standards for an ideal IDD formulation, as outlined by a panel of IDD experts9. It has demonstrated safety and efficacy in clinical studies in infants as young as 3 months, with comparable efficacy to ZnO lipophilic paste. Furthermore, it is appropriate for repeated daily administration to the still maturing and sensitive skin of young infants due to its convenient formulation, free from perfumes and anti-septics. Moreover, the formulation leaves only a transparent layer on the skin making it easy to assess the skin status of the infant buttocks in contrast to ZnO lipophilic pastes which often leaves a white, adherent layer on skin.
Correspondence to: Holger Lenz, Bayer Consumer Care, Peter-Merian-Strasse 84, CH-4052 BASEL, Switzerland.
Disclosures: The authors were all involved in the design, methodology, analyses and interpretation of the data presented in this article. Raymond de Bony, Peter Kurka, and Holger Lenz are all employees of Bayer Consumer Care AG, Basel, marketing Bepanthen Extra Protection. Katarzyna Sznurkowsk and Anna Liberek are employees of Dermscan Poland conducting the cosmetic tests.
Acknowledgements: We would like to acknowledge the editorial assistance of Dr. Stuart Marshall of Core Medica Ltd., a Division of the Prime Medical Group, in the development of this manuscript, as well as the technical expertise and support of Armelle Magnet, Sandrine Botalla and Delphine Rochot, International Technology Centre, Bayer Consumer Care, Gaillard, France.
References
- Atherton DJ. A review of the pathophysiology, prevention and treatment of irritant diaper dermatitis. Curr Med Res Opin. 2004;20:645–649.
- Benjamin L. Clinical correlates with diaper dermatitis. Pediatrician. 1987;14 Suppl 1:21–26.
- Yadav M, Singh PK, Mittal SK. Variation in Bowel Habits of Healthy Indian Children Aged up to Two Years. Indian J Pediatr. 2013;
- Jordan WE, Lawson KD, Berg RW, Franxman JJ, Marrer AM. Diaper dermatitis: frequency and severity among a general infant population. Pediatr Dermatol. 1986;3:198–207.
- Atherton DJ. The aetiology and management of irritant diaper dermatitis. J Eur Acad Dermatol Venereol. 2001;15 Suppl 1:1–4.
- Stamatas GN, Nikolovski J, Luedtke MA, Kollias N, Wiegand BC. Infant skin microstructure assessed in vivo differs from adult skin in organization and at the cellular level. Pediatr Dermatol. 2009;27:125–131.
- Nikolovski J, Stamatas GN, Kollias N, Wiegand BC. Barrier function and water-holding and transport properties of infant stratum corneum are different from adult and continue to develop through the first year of life. J Invest Dermatol. 2008;128:1728–1736.
- Atherton D, Mills K. What can be done to keep babies' skin healthy? RCM Midwives. 2004;7:288–290.
- Atherton D, Proksch E, Schauber J, Stalder J. Irritant Diaper Dermatitis: Best Practice Management. SelfCare 2015;6(S1):1-11.
- Coppi G, Bonardi G. Urease-inhibiting action of some drugs in vitro and in vivo. Arzneimittelforschung. 1970;20:384–386.
- Tanno O, Ota Y, Kitamura N, Katsube T, Inoue S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability barrier. Br J Dermatol. 2000;143:524–531.
- Bissett DL. Common cosmeceuticals. Clin Dermatol. 2009;27:435–445.
- Biro K, Thaci D, Ochsendorf FR, Kaufmann R, Boehncke WH. Efficacy of dexpanthenol in skin protection against irritation: a double-blind, placebo-controlled study. Contact Dermatitis. 2003;49:80–84.
- Camargo FB, Jr., Gaspar LR, Maia Campos PM. Skin moisturizing effects of panthenol-based formulations. J Cosmet Sci. 2011;62:361–370.
- British Standards Institute. Test Methods for Primary Wound Dressings. Moisture Vapour Transmission Rate of Permeable Film Dressings. B S I Standards; 2002.
- Patton CJ, Crouch SR. Spectrophotometric and kinetics investigation of the Berthelot reaction for the determination of ammonia. Anal Chem. 1977;49:464–469.
- Couarraze G, Grossiord JL. Initiation á la rhéologie. Lavoisier; 1983.
- Marzulli FN, Maibach HI. The use of graded concentrations in studying skin sensitizers: Experimental contact sensitization in man. Food and Cosmetics Toxicology. 1974;12:219–227.
- Human Experimentation: Code of Ethics of the World Medical Association (Declaration of Helsinki). Can Med Assoc J. 1964;91:619–
- Fitzpatrick TB. The validity and practicality of skin types I through VI. Arch Dermatol. 1988; 124: 869-871
- Putet G, Guy B, Andres P et al. Effect of Bepanthen ointment in the prevention and treatment of diaper rash on premature and full-term babies. Réalités Pédiatriques 2001;63:33-38.
- Gehring W, Gloor M. Effect of topically applied dexpanthenol on epidermal barrier function and stratum corneum hydration. Results of a human in vivo study. Arzneimittelforschung. 2000;50:659–663.
- Cork MJ, Danby SG, Vasilopoulos Y, Hadgraft J, Lane ME, Moustafa M, Guy RH, Macgowan AL, Tazi-Ahnini R, Ward SJ. Epidermal barrier dysfunction in atopic dermatitis. J Invest Dermatol. 2009;129:1892–1908.
- Lawton S. Skin barrier function and the use of emollients in dermatological nursing. Br J Nurs. 2007;16:712–719.
- Proksch E, Lachapelle JM. The management of dry skin with topical emollients--recent perspectives. J Dtsch Dermatol Ges. 2005;3:768–774.
- Proksch E, Brandner JM, Jensen JM. The skin: an indispensable barrier. Exp Dermatol. 2008;17:1063–1072.
- Telofski, LS, Morello, AP, III, Mack Correa, MC, Stamatas, GN. The infant skin barrier: can we preserve, protect, and enhance the barrier? 2012. Last accessed on 23 December 13 A.D.
Reference Link - Bikowski, J. Update on Prevention and Treatment of Diaper Dermatitis. 2011. Last accessed on 23 April 14 A.D.
Reference Link - Heisterberg MV, Menne T, Johansen JD. Contact allergy to the 26 specific fragrance ingredients to be declared on cosmetic products in accordance with the EU cosmetics directive. Contact Dermatitis. 2011;65:266–275.