INTRODUCTION
The commonest causes of acute ‘red eye’ (inflamed conjunctiva) are self-limiting or amenable to simple self care measures. When health care professionals are consulted, it is helpful to use the opportunity to educate consumers on the measures they can safely take themselves and, just as importantly, the symptoms and signs that should lead them to seek professional advice promptly.
Some categories of patients need special attention and may not be suitable for self-care at all.
The causes of red eye include some serious conditions (such as iritis) that can threaten sight if managed inappropriately. However, if consumers follow simple rules, these more serious but rarer causes can be identified early and specialist review can be expedited.
Consumers may present after self-treating with ophthalmic preparations available in pharmacies and these may actually contribute to symptoms in some circumstances. Persistent symptoms or failure to respond promptly to self care measures should always lead to consultation and the ‘self care history’ can help to guide further management.
ACUTE ‘RED EYE’
WHEN SELF CARE IS NEVER APPROPRIATE
An important objective in guiding self care of red eye is to ensure that consumers recognise the circumstances when professional clinical help is always required. Fortunately, guidance familiar to general practitioners1,2 can be readily adapted to guide consumers.
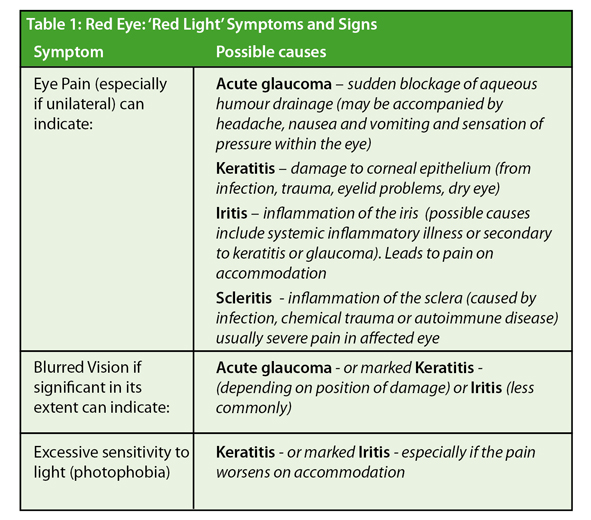
There are three important symptoms that indicate a possible serious cause and should always lead to prompt consultation (Table 1). Severe unilateral red eye (especially if accompanied by one of these additional symptoms) should also be regarded as a reason for examination by a physician.
Other causes of ‘localised’ red eye such as subconjuntival haemorrhage or episcleritis are generally also worthy of a medical assessment and opinion on the first occurrence to ascertain the underlying cause, if any.
CATEGORIES OF CONSUMERS INAPPROPRIATE FOR UNSUPERVISED SELF CARE:
Any history suggestive of physical or chemical trauma
Many consumers engage in activities (e.g. Do-it-Yourself home improvements) that risk eye trauma of various kinds. Chemical contamination of the eye (e.g. with irritants such as Alkalis e.g. wet cement) or acids is usually painfully obvious. To minimize damage undertake Cand copious irrigation of the eye while expert help is sought
Symptoms of physical trauma can also be obvious but sometimes misleading. If there is a history of trauma leading to a red eye of any severity the sufferer will require a prompt examination of the eye. Use of hammer and chisel hand tools or power tools without eye protection can cause projectile foreign bodies to impact in the conjunctival space or damage the cornea. High velocity fragments can even cause unsuspected penetrating injury. Direct blunt trauma to the eye can likewise lead to unsuspected damage of internal ocular structures.
Therefore red eye caused by chemical or physical trauma should not be managed by self care without professional advice.
Contact lens use
Contact lens users are at a higher risk of developing aggressive bacterial infections, and associated keratitis or a corneal ulcer, than those who do not wear them. Pseudomonas aeruginosa infections are more common in lens users. Chloramphenicol (the only antibiotic eye drops currently available for self care in pharmacies in the UK) is not suitable for infections caused by this pathogen. Additionally, contact lens use can impair corneal sensitivity and therfore wearers may not always feel pain early in the course of a potentially serious infection.
For these reasons contact lens users should never self medicate for red eye. General Practitioners have a low threshold for referral to opthamic specialists those lens wearers who present with apparent bacterial infections.
Herpes Simplex or Zoster skin lesions
A history of recent skin spots and raches similar to cold sores followed by red eye, may indicate herpetic keratitis. Ophthalmic examination with fluorescein is required to look for the branching or ‘dendritic’ corneal ulcers typical of the condition.
Red eye associated with shingles affecting the face might indicate herpes zoster ophthalmicus. Shingles affecting the skin served by the first division of the trigeminal nerve, particularly if the tip of the nose is affected, indicates a significant risk that the eye will be affected.
Therefore people developing red eye associated with any herpetic-type lesions affecting the face or scalp should not self treat without advice.
COMMON CAUSES OF RED EYE
Infectious Conjunctivitis – clinical features
The commonest cause of red eye is an infectious conjunctivitis; with viral and bacterial pathogens accounting for approximately half of the infections each. Whether viral or bacterial, the majority of cases of infectious conjunctivitis are self limiting.
The typical features of infectious conjunctivitis are generalised redness and injection (redness and swelling) of the conjunctivae (most usually bilaterally) accompanied by a discomfort often characterised as ‘grittiness’, and a discharge from the eyes. Importantly, vision is not affected (other than by the discharge) and remains clear. The eyes are not painful, and photophobia is not a feature.
It is not possible to distinguish reliably between viral and bacterial infections on symptoms alone. However bacterial infections are said to be more often associated with bilateral gluing of the eyes by discharge on waking in the morning. Generally viral infections are said to produce a more watery and mucoid discharge (rather than the frankly purulent discharge typical of a bacterial infection). A recent history of an upper respiratory tract infection may also be present if the origin is viral. If consumers are alerted to the clues (e.g. a recent cold) that particularly suggest a viral origin, this may help to reduce unnecessary antibiotic usage.
Viral infections tend to run a more prolonged course than bacterial ones, often lasting several weeks. More unusual infections can occur. For example mild and persistent symptoms in young sexually active people can indicate Chlamydia as a cause, particularly if the symptoms are unilateral. Allergic conjunctivitis is generally associated with minimal discharge but prominent itchiness and may cause bilateral red eye for as long as the allergen is present. This diagnostic uncertainty, and the advantages of identifying the allergens causing the reaction, means that persistent symptoms are best reviewed by a doctor.
Management of infectious conjunctivitis
Self care of infectious conjunctivitis should be encouraged if symptoms are typical and none of the ‘alarm’ features above are present. Consumers need to know that the condition is self-limiting in most cases, so that they can make informed choices about the use of topical antibiotics.
General Advice
• Infectious conjunctivitis is highly contagious and people must wash their hands frequently, particularly after dealing with secretions. Infected individuals should not share towels or bed linen.
• Infected secretions (which can be sticky and adherent to lashes) may be gently removed by washing with cotton wool soaked in sterile water. Warm water compresses can be used to soften secretions that have hardened overnight.
• The gritty discomfort can be eased by lubricant eye drops readily available from pharmacies.
• Regular contact lens wearers should not self-medicate (see above) but contact lens use must be discontinued in any active case of red eye.
Use of antibiotic drops
Chloramphenicol eye drops are available in UK pharmacies as ‘P’ medicines (to be sold under the supervision of a pharmacist) for the treatment of acute bacterial conjunctivitis. Consumers need to be aware that about half of infectious conjunctivitis cases will be viral and that bacterial conjunctivitis is self-limiting in most cases if left untreated. A Cochrane review of studies that compared use of antibiotics with placebo for acute bacterial conjunctivitis found that antibiotics resolved symptoms more quickly but that the benefit was marginal3.
Many general practitioners suspecting a bacterial cause will issue a prescription for a topical antibiotic but suggest that patients delay treatment for up to a week – to allow an opportunity for symptoms to resolve spontaneously4. A similar approach can be suggested to individuals considering self care with an antibiotic preparation. Pharmacists should reassure consumers that the risk of serious complications from infectious conjunctivitis left untreated by antibiotics is very low.
People self medicating with chloramphenicol eye drops are advised that if their symptoms do not improve in 48 hours or if they persist after the recommended 5 day course, they should consult a doctor. Causes of persistent symptoms after chloramphenicol drops include sensitivity to the drug or the preservative in the drops – so consumers should be advised to stop the treatment while waiting to see their doctor.
CONCLUSION
Acute red eye is a frequent cause of presentation to a general practitioner. The common causes of red eye are suitable for self care provided that the consumer is alert to the ‘alarm symptoms’ which indicate the need for expedited review. Some categories of patients with red eye (e.g. those with symptoms after injury or contact lens users) should never self medicate without a prior examination and medical advice.
In many cases, simple eye hygiene and symptomatic treatment will be sufficient while the condition resolves spontaneously. Consumers should be given adequate information to allow them to make an informed choice regarding the use of topical antibiotics for self care. Persistent symptoms or failure to respond to self medication bring a wider range of diagnostic possibilities into consideration and the self care history can be helpful in guiding next steps.
Correspondence to: Dr James Kennedy c/o editor@selfcarejournal.com
Conflict of Interest Statement: None.
References
- NHS Clinical knowledge summary : Red Eye. https://www.cks.nhs.uk/red_eye (Accessed 11th August 2010).
Reference Link - NHS Clinical knowledge summary : Infectious Conjunctivitis. https://www.cks.nhs.uk/conjunctivitis_infective (Accessed 11th August 2010)
Reference Link - Sheikh, A. and Hurwitz, B. (2006) Antibiotics versus placebo for acute bacterial conjunctivitis (Cochrane Review). The Cochrane Library. John Wiley & Sons, Ltd. www.thecochranelibrary.com [Free Full-text] Accessed 11th August 2010
Reference Link - Everitt, H.A., Little, P.S. and Smith, P.W. (2006) A randomised controlled trial of management strategies for acute infective conjunctivitis in general practice. British Medical Journal 333(7563), 321. https://www.ncbi.nlm.nih.gov/pubmed/16847013
Reference Link