INTRODUCTION
Sore throat is one of the commonest minor ailments presented to general practitioners. Often these consultations result from the still prevalent belief that antibiotics are necessary to speed recovery. In reality most sore throats are caused by viral pathogens and run a benign, self-limiting course. It is important that sufferers understand the limited place of antibiotics (including the associated disadvantages) in the treatment of bacterial sore throat, and this understanding is necessary to underpin the current practice of issuing delayed prescriptions for antibiotics.
More serious causes of sore throat are uncommon but it is useful to remind people of the signs and symptoms that indicate the need for professional assessment (e.g. persistent high temperature) or that constitute rare medical emergencies (e.g. difficulty breathing or swallowing saliva) presenting in this way.
Some patients, such as those with immune systems compromised because of disease (e.g. HIV infection) or drug therapy (e.g. disease modifying agents for rheumatoid arthritis), should always consult rather than self-medicate.
Sore throat symptoms can be managed by simple measures (such as oral analgesics and anti-inflammatory drugs) and avoiding exacerbating factors (such as hot drinks). Many medicinal products are available for the self-medication of sore throat, but the evidence base for some of the older topical remedies is weak or lacking.
ACUTE SORE THROAT1
CONSULTATION GUIDANCE
Sore throats are most commonly associated with viral infections such as the common cold or influenza. In these cases there is often a history of similar symptoms in the family or other contacts. If people with simple viral sore throat examine their pharynx in the mirror, redness or swelling is usually minor, if present at all.
Other less common viral causes include infectious mononucleosis (glandular fever), when fever and cervical lymphadenopathy are prominent and malaise is often marked. This should be suspected if the sore throat fails to improve or gets worse over several days.
It is usually not possible to determine the cause of sore throat, and in particular to distinguish bacterial causes (the commonest being streptococcal infection) from the much more common viral infections. For this reason, unless there are clear reasons for concern (such as a high temperature, or symptoms worsening rather than improving over a few days, or persisting longer than a week) consultation with a doctor is not normally necessary, particularly since investigations and antibiotics are not indicated.
In contrast, people should be aware that there are circumstances in which urgent medical advice or even urgent hospital admission is necessary (Table 1).

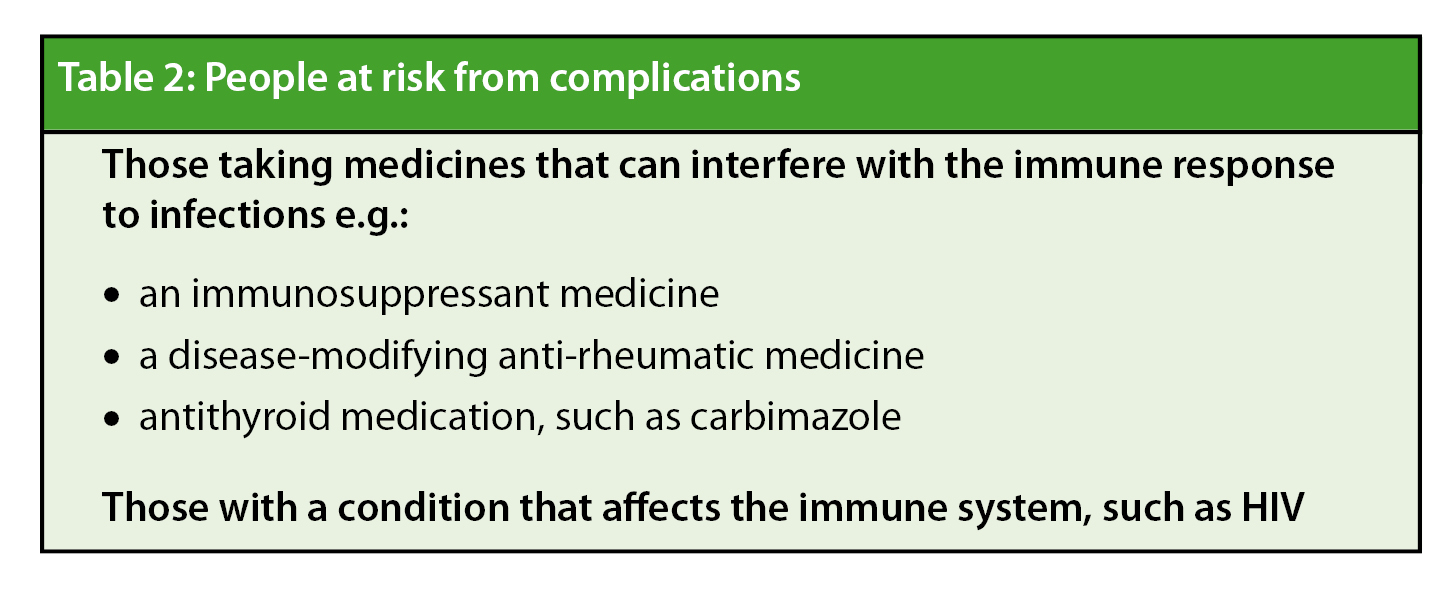
There are also groups of patients that should not self-medicate for sore throat since they are at risk of complications either from an adverse effect of a medication they are taking or as a result of an underlying condition causing immune suppression (Table 2).
SELF CARE ADVICE
People can obtain some relief from acute sore throat by adopting simple self care measures:
• Avoiding irritant foods or hot drinks
• Mouthwash or gargling with warm slightly salty water
• Sucking sweets, lozenges or ice to provide some direct soothing effect.
People should be encouraged to maintain an adequate fluid intake, particularly if they have fever, so as to avoid becoming dehydrated.
Regular use of oral analgesics such as paracetamol or ibuprofen will help to control discomfort and will also reduce fever if present. Some local analgesics, delivered as throat sprays, gargles or lozenges, are available as non-prescription medicines, however evidence to support additional benefit over simple measures is lacking.
ANTIBIOTICS IN SORE THROAT
Antibiotics should only become an option for treating sore throat if people consult a doctor. However surveys have shown that consumers may use hoarded drugs for self care2, so it is important to emphasise the limited place that antibiotics have in treating sore throat. There is evidence that many people with sore throat consult for reassurance3, and the self-limiting nature of symptoms without resort to antibiotics is worth emphasis to guide self care in future episodes.
Even if symptoms and signs suggestive of a bacterial cause for sore throat are present (the Centor Criteria, Table 3), the evidence suggests that antibiotic treatment only shortens the duration of symptoms modestly4. For this reason, a delayed prescription for antibiotics may be issued in those with a high likelihood of bacterial infection – with the prescription to be used only if symptoms worsen within 3 days or fail to improve after 3 days. This ‘deferred self care’ with antibiotics relies on consumer understanding of the rationale behind limiting antibiotic usage. There is some evidence from a UK study that delayed antibiotic prescribing may reduce re-attendance rates5.

CONCLUSION
Sore throat is one of the commonest reasons for people in the UK to consult a doctor. In the majority of cases this consultation achieves little more than reassurance that the symptom will resolve on its own. As with many common minor ailments, experience and education are important in arming people to self care in most circumstances.
Persistent high temperature, difficulty swallowing and any suggestion of difficulty breathing should prompt urgent consultation and there are some patient categories (e.g. those with disease or drug induced immune suppression) that should not manage sore throat without advice. However sore throat is most often part of a viral infection and a combination of analgesics and antipyretics with simple measures to soothe local discomfort are all that is needed.
Even when bacterial infection is more likely to be the cause of sore throat, antibiotics have a limited place in treatment of this often self-limiting symptom. It is now common practice for general practitioners not to offer antibiotics at all or to defer supply until symptoms worsen or fail to improve after a few days. For these strategies to succeed in the aim of reducing unnecessary antibiotic usage it is crucial to explain why they are being adopted. Use of hoarded drugs or those acquired from other sources (such as relatives) may result from an incomplete appreciation of the risks or unrealistic expectations of the benefits of antibiotics for sore throat.
Correspondence to: Dr James Kennedy c/o editor@selfcarejournal.com
Conflict of interest statement: none
References
- NHS Clinical knowledge summary : Acute Sore Throat. https://www.cks.nhs.uk/sore_throat_acute (Accessed 10th January 2011).
Reference Link - Grigoryan L, Haaijer-Ruskamp FM, Burgerhof JG et al., Self-medication with antimicrobial drugs in Europe. Emerg Infect Dis. 2006 Mar;12(3):452-9.
Reference Link - van Driel, M.L., De Sutter, A., Deveugele, M. et al. (2006) Are sore throat patients who hope for antibiotics actually asking for pain relief? Annals of Family Medicine 4(6), 494-499.
Reference Link - Del Mar, C.B., Glasziou, P.P. and Spinks, A.B. (2006) Antibiotics for sore throat (Cochrane Review). The Cochrane Library. Issue 4. John Wiley & Sons, Ltd.
Reference Link - Little, P., Gould, C., Williamson, I. et al. (1997a) Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. British Medical Journal 315(7104), 350-352.
Reference Link
Reference Link