INTRODUCTION
Headache is one of the commonest conditions that people treat without professional advice. Most common causes of intermittently recurrent headache are adequately treated with simple analgesics and cause little concern to the sufferer. However, when symptoms become more frequent or severe and sufficient to interfere with daily life, advice on appropriate self-medication may be sought.
Most self care of headaches takes place in response to symptoms with an established and familiar pattern. If the frequency is low and the symptoms are not disabling and easily managed with simple analgesia, then professional help is seldom sought. Headaches that disrupt normal life and interfere with work or study are more often of concern and family or friends may urge medical consultation.
One of the commonest questions posed is: ‘is it migraine?’ People may label any severe headache ‘migraine’ but the distinction between migraine and other recurrent headaches is not based solely on severity, and has implications for self management.
A careful review of recurrent headache in sufferers may identify possible triggers in their daily lives that contribute to their problem. An example of frequent recurrent headache is medication overuse headache (MOH). Awareness of MOH in the general public is low, and this condition, as its name implies, is an important challenge arising from both self care and prescribed medication treatment of headache. A large reduction or even complete withdrawal of analgesics will yield a marked improvement in symptoms.
Headache may be the presenting symptom of a wide range of conditions from mild self limiting to very serious. Serious secondary causes of headache include: trauma, intra-cerebral haemorrhage, inflammation of the brain or meninges (covering of the brain), infection, malignancy, glaucoma and carbon monoxide poisoning. Any new headache with new features, and particularly those with associated signs and symptoms (e.g. fever, nausea, impaired consciousness or other neurological signs) should be promptly medically assessed for secondary causes.
‘IS IT MIGRAINE?’
Migraine and tension type headache (TTH) are the commonest types of recurrent primary headache. Distinguishing between the two on symptomatic grounds may be straight forward if symptoms are entirely typical1,2 but more often a ‘pattern’ needs to develop with recurrent episodes (Table 1).
Table 1: Characteristic Features of Primary Headache Types*
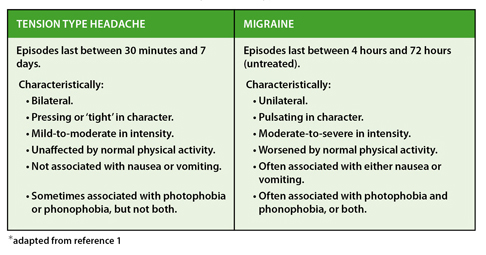
Migraine is a chronic condition, affecting approximately 10-15% of adults and often starting in adolescence and developing into a repeating pattern of symptoms. It is more common in women and there is often a positive family history. In around 25% of sufferers the headache of migraine is preceded by reversible neurological symptoms or ‘aura’ (particularly visual but sometimes sensory symptoms or dysphasia), however the majority have no such warning symptoms. The frequency and nature of attacks varies widely between individuals, but between one and four episodes per month is typical.
When typical features of migraine are present, specific treatments may be suitable, particularly when simple analgesics are insufficient to control symptoms. In several European countries, (Germany and UK) drugs of the triptan class are available for self care of established migraine.
The ‘triptans’ are all selective 5-HT 1B/1D agonists and cranial vasoconstriction and peripheral trigeminal inhibition may contribute to their action. These drugs can be particularly helpful when taken early in an attack. Sumatriptan (in the UK) and naratriptan (in Germany) are available for purchase from pharmacies for suitable individuals.
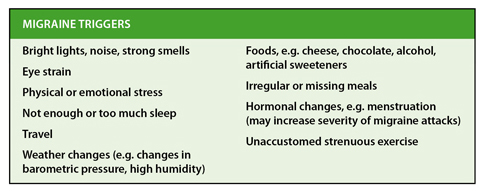
In most migraine sufferers the attacks follow a pattern: a recurring pounding headache, associated with nausea and visual symptoms and often with one or more ‘triggers’ that appear to precipitate attacks. Some of these may be avoidable (see Table 2 for some examples).
Awareness of these triggers, perhaps through keeping a diary, may be a good starting point for self care. However it is important to appreciate that triggers are specific to individuals, so not all migraine sufferers need to abstain from chocolate and cheese, for example.
Table 2: Commonly Reported ‘Migraine’ Triggers
HEADACHE TRIGGERS AND CAUSES
The presence of a recognisable trigger for an individual’s headaches is not by itself diagnostic of migraine. Food triggers are more common in migraine, but other precipitants of headaches (such as tiredness or emotion) are present equally in TTH and migraine3.
Individuals may need to be reminded that headaches can result from caffeine withdrawal (if they are regular consumers of caffeinated drinks such as coffee and tea and their normal routine is interrupted) or missing meals or fluids. Many medications have been reported to cause headache as an adverse event, so recent changes in prescription or self medications may be to blame if headaches become more of a problem than is usual for an individual.
MEDICATION OVERUSE HEADACHE (MOH)
Very high proportions of people with TTH or migraine take regular prescription medicines or purchased analgesics, or both. If headaches are frequent, or inadequately managed, frequent consumption of treatments can lead to additional problems. Medication Overuse Headache should be suspected if headache symptoms develop into a chronic pattern, with symptoms on more than 15 days a month, while medication is being taken frequently2,4.
The population-based prevalence of MOH is 0.7% to 1.7% and it may complicate an underlying headache arising from a different cause. MOH can occur with both TTH and migraine (although it is more common with the latter) and with any headache medication, including specific migraine treatments. Typically, the symptoms of MOH resemble those of the original condition treated – so people are more likely to develop migraine-like MOH on triptans, for example. People with migraine or TTH may develop MOH if they take analgesics frequently for other non-headache chronic pain.
Although MOH will normally resolve on withdrawal of the drug treatment causing the headache, this withdrawal may be difficult to achieve as sufferers may be reluctant to stop their medications. In any event a review of the underlying condition and its treatment is always warranted when a treatment needs to be excessively frequent. In migraine, once MOH has resolved, it may be necessary to consider preventative therapy.
CONCLUSION
Headache is one of the commonest reasons for self medication. In general, self care with simple analgesics is all that is required for most people most of the time and there is only a need for professional help when symptoms become unmanageable by these means.
If headaches become frequent or disabling in severity, a definite diagnosis is very helpful, not least because specific treatment (e.g. for migraine) can make a considerable difference to the quality of life for sufferers. Triptan drugs for established migraine symptoms are now available for pharmacist supervised purchase in several European countries. The recognition of common patterns of symptoms and the environmental triggers relevant to the individual can improve self care of both migraine and TTH.
Importantly, consumers should be educated to recognise that new or significantly changed symptoms, particularly those with associated symptoms such as fever or neurological signs, should prompt early consultation with a doctor.
Finally the message that frequent use of medication can itself cause chronic headache symptoms deserves to be better known in the public at large, particularly now that self care of migraine with triptans is possible.
Correspondence to: Dr James Kennedy c/o editor@selfcarejournal.com
Conflict of Interest Statement: None.
References
- NHS Clinical knowledge summary : Headache Assessment. https://www.cks.nhs.uk/headache_assessment (Accessed 12th November 2010).
Reference Link - BASH (2007) Guidelines for all healthcare professionals in the diagnosis and management of migraine, tension-type, cluster and medication-overuse headache. British Association for the Study of Headache. Accessed 12th November 2010
Reference Link - Smetana GW. The diagnostic value of historical features in primary headache syndromes: a comprehensive review. Arch Intern Med. 2000 Oct 9; 160(18):2729-37. Review.
Reference Link - Evers S, Marziniak M. Clinical features, pathophysiology, and treatment of medication-overuse headache. Lancet Neurol. 2010 Apr; 9(4):391-401.
Reference Link