Abstract
background
There is resurgent interest in the concept and practice of self-care as a means to improve the health, wellness and wellbeing of individuals, and as an avenue to mitigate financial pressures and growing demands on health and social care systems worldwide. An ongoing challenge has been the lack of clarity on the specific nature and entire scope of self-care, coupled to a lack of a universal or widely accepted framework that could support the conceptualisation and study of self-care in its totality, in all settings and from different perspectives.
objectives
To advance a comprehensive yet pragmatic and widely accessible framework to support the conceptualisation of self-care in its totality, in order to facilitate the development, commissioning, evaluation and study of self-care initiatives across a variety of settings.
Method and framework development
A pragmatic review of the academic and lay literature was undertaken to identify extant theories and conceptual models of self-care. Following a content analysis, the models were characterised, and a configuration matrix was constructed to illustrate the key components and main themes of each model. These themes were organised into a number of domains which were grouped together into cardinal dimensions of self-care. The dimensions of self-care were consolidated in an inclusive framework and visually depicted on a schema to illustrate their inter-relationship.
results
We identified a total of 32 candidate models, theories and frameworks of self-care. Characterising these models led to the identification of various themes and domains. These were found to naturally group into four cardinal dimensions of self-care: (1) Activities, (2) Behaviours, (3) Context, and (4) Environment. A new model was synthesised to illustrate the relationship between each dimension on a configuration matrix resulting in the creation of the Self-Care Matrix (SCM).
conclusion
The Self-Care Matrix (SCM) is a useful framework that can be used to conceptualise and frame the totality of self-care and its various interlinked elements. SCM is intended for use by all stakeholders who are interested in the study, development, commissioning and evaluation of self-care initiatives.
Full text
introduction
The global epidemic of long-term noncommunicable diseases (NCDs) and so called ‘lifestyle diseases’ observed today is a direct result of our inability to self-care1,2. Consequently, policymakers and commissioners of health services in England and elsewhere are increasingly looking at self-care initiatives as a potential means of promoting health and wellbeing in individuals and communities, whilst reducing costs and demand on scarce national healthcare resources.
There are many potential policies which support self-care activities and the sustained adoption of positive lifestyle behaviours in everyday life. However, because existing self-care interventions are usually linked to a general disease area or the management of a specific condition3, there is scant evidence on the cost-effectiveness of self-care interventions across different settings4-6. An additional barrier to the widespread adoption of self-care initiatives is the lack of a suitable model to support the conceptualisation of self-care in its totality, explaining the relationship between self-care activities and behaviour change in the context of resource utilisation, and how self-care praxis can be modulated by external forces and the wider environment.
A recent study identified over 136 definitions of self-care7, with various terms including ‘self-management’, ‘self-efficacy’, ‘self-treatment’ and ‘collaborative care’ often used interchangeably8-10 depending on the correlating theories and the academic field of interest7,11-16. Consequently, various definitions of self-care have emerged as a result of differing perspectives between healthcare professionals and the general public, and between health professionals in different disciplines7.
Various instruments have been used to assess proxy measures of self-care capacity and capability17-19, including the Patient Activation Measure (PAM)20-22. However, health and social support concepts such as self-care are generally less amenable to direct measurement and evaluation due to a lack of efficient indicators23-26 and the wide potential range of measurables. Because self-care is intimately linked to behaviour change theory which merges the fields of sociology and psychology and refers to a mutation in human health behaviour29,30, any measurement related to self-care, either as a concept or a set of actions or behaviours, is also dependent on the specific impairment perspective27,28. Thus, whereas several existing frameworks and models can be used to explore the relationship between self-care and behaviour change31-48, there is currently no univocal definition of self-care, no instrument that can measure the totality of self-care indicators directly, and no candidate model or unifying framework that can be used to explicate self-care in its totality.
Conceptualising self-care
Godfrey identified various models of self-care from the academic literature13, but her seminal analysis excluded the study of other widely accepted but non-academic conceptual models of self-care. For example, there exist in the lay literature a number of alternative yet non-mutually exclusive mid-level descriptions and conceptual models to support the study and application of self-care in various settings. These include: (1) the widely used Seven Pillars of Self-Care Framework49 which describes the main activities and elements of self-care relevant to the individual self-carer, and (2) the Self-Care Continuum50 which describes the placement of an individual along a continuum of care in the context of resource utilisation. However, neither model from academic or lay literature was developed specifically for the purpose of conceptualising self-care in its totality, or could explain the link between self-care activities, behaviour change and resource utilisation in the context of the prevailing culture and the external environment. The lack of a conceptual and unifying framework that attempts to capture the totality of self-care may impede the development and deployment of self-care initiatives in the contemporary setting.
Aim
To characterise and consolidate existing models of self-care theory and practice gleaned from both academic and lay literature to advance a comprehensive yet pragmatic framework that facilitates the conceptualisation of self-care in its totality and its study across all settings.
Methods
Pragmatic review of the literature
A pragmatic review of the literature was conducted to identify published theories linked to self-care and relevant models and frameworks used to conceptualise self-care across various settings. We conducted searches based on titles on all relevant databases including MEDLINE; Embase; HIMIC; Global Health; and PsychINFO through Ovid. The initial search identified 752 publications for the period 1983-2018. Additionally, we searched on CINAHL, Scopus and Cochrane databases which revealed 436, 563 and 68 publications respectively. The search in all databases used the terms: self care, self monitoring and self management to identify the relevant articles. The results of each category were combined using Boolean terms ‘AND’ and ‘OR’ to narrow down the search findings after linking with keywords like “model*”, “framework*” and “scheme*”. We also included relevant models and frameworks gleaned from non-academic literature including websites of various non-governmental organisations, charities and other entities engaged in the self-care discourse such as the World Health Organisation (WHO), Kaiser Permanente, the Self-Care Forum UK and the International Self-Care Foundation.
Characterising self-care models and theories
An initial review of single-disease specific models and frameworks aimed at explaining self-care theory and praxis was undertaken, which resulted in a list of 631 manuscripts. After scanning this list, a total of 44 papers were found to pertain to self-care models, frameworks, concepts or theories. This initial list included various examples of how self-care links with behaviour change theory (n=12). The latter were excluded, and the final list (n=32) was used to characterise various aspects of each self-care model.
Framework synthesis
A qualitative content analysis approach was used to identify the key assumptions, characteristics, themes and domains of self-care pertaining to each model. Further to characterising each model, we identified a number of themes and perspectives which could be conveniently grouped into various domains. These domains were found to naturally group together under four cardinal ‘dimensions’ of self-care. The inter-relationship between each self-care dimension was considered. A visual depiction of each dimension was juxtaposed on a matrix resulting in a schema of the newly synthesised framework that could be used to conceptualise self-care theory and practice in its totality. The resulting unifying framework (the Self-Care Matrix) was assessed for congruence by determining the extent to which it supported the formal study of self-care as an applied field of research, whilst providing a logical connection between each dimension.
results
Characterising existing models and concepts of self-care.
Table 1: Characteristics of 32 generic theories, models and frameworks associated with self-care.

Our pragmatic review of lay and academic literature identified a range of perspectives on self-care in various contexts. We identified and characterised 32 different theories, models and frameworks that attempted to describe self-care from different perspectives. Table 1 summarises the key points of the most relevant theories and models of self-care, grouped as either prevention-focused (n=9), rehabilitation-focused (n=16) or concerned with both prevention and rehabilitation (n=7). Theories ranged from academic theories illustrating the antecedents (i.e. aspects necessary for the performance) and the consequences (i.e. results of the performance) of self-care, to more applied concepts that supported the understanding of self-care in the context of resource utilisation, or applied interventions for behaviour change in autonomous or assisted care settings.
Table 2: Characteristics of the four cardinal dimensions of self-care

The four cardinal dimensions of self-care
Content analysis and characterisation of each model resulted in the identification of various themes and domains of self-care which could be naturally grouped under four dimensions of self-care (table 2). The four cardinal dimensions of self-care identified were: (1) Self-Care Activities, (2) Self-Care Behaviours, (3) Self-Care Context, and (4) Self-Care Environment (table 2). Each dimension pertains to a different aspect of self-care as follows:
1st Dimension: Self-care activities (micro-level: person-centred)
The first dimension is concerned primarily with individual activities, capacities and capabilities, and what people know and do to self-care. At this micro-level, self-care is considered from a person-centred perspective. Suitable interventions may be developed to improve and promote health maintenance, monitoring and self-management of common, every-day or long-term conditions. The Health Belief Model, Orem’s Self-Care Deficit Nursing Theory51-53, and the widely used Seven Pillars of Self-Care model54 are suitable candidate models that can be used to explore this cardinal dimension. The first dimension of self-care is necessarily concerned with the ‘self’, is person-centric and activities therein relate directly to what individuals can do for themselves, as well as the knowledge required to inform suitable self-care choices, such as health literacy and self-awareness.
2nd Dimension: Self-care behaviours (meso-level: Individual and group focused)
The second dimension is concerned with the principles and actions that support and motivate individuals to engage in positive self-care behaviours and achieve the sustained adoption of health-seeking behaviours and lifestyles choices. Interventions operating at this meso-level include efforts to improve PAM scores, the use of digital health technology including nudges, gamification an incentivisation strategies to promote the sustained adoption and maintenance of desirable lifestyle choices and habits. Associated theories include the Middle Range Theory of Self-Care55 which addresses health promoting practices within the context of the management of a chronic illness. The widely used trans-theoretical model of behaviour change and the Behaviour Change Wheel48 are suitable candidate models that adequately describe activation and behaviour change elements relevant to self-care. The second dimension is focused on the individual, but may also extend to the social network as it describes the prevailing ‘lifestyle’ habits, normative attitudes and routine interactions with the immediate environment, including interface with technology and decision support tools.
3rd Dimension: Self-care context and reliance on resources (meso-level: patient-centred, health system focused)
The third dimension considers the extent to which an individual is reliant on external resources in the home, community, assisted care or professional healthcare settings. Interventions at this meso-level are often health system-focused, whereby an individual, a demography or a segment of society is routinely considered from a ‘statist’ or medicalised patient-perspective as opposed to a person-centred perspective. Interventions at this level are often concerned with modulating resource utilisation, including access to services, clinical pathways and/or the extent of integration of care. The widely used Self-Care Continuum54 and the Kaiser Permanente Pyramid of Self-Care model56 are suitable candidates for this dimension as they dynamically illustrate the inverse relationship between individual autonomy and reliance on external resources or need for increasing support.
4th Dimension: Self-care environment, barriers and drivers to self-care (macro-level: policy-driven, health system focused)
The fourth dimension is concerned with existing drivers and barriers to self-care in relationship to the operating fiscal and policy environment, and in the context of the prevailing culture and normative attitudes that inform self-care praxis in the wider community. This dimension takes into account the built and natural environment and other mediating factors. At this macro-level, drivers and barriers to self-care operate at scale or at population level. The fourth dimension is thus related to the public health landscape and informs the ‘country narrative for self-care’, which is largely influenced by the prevailing cultural and societal attitudes and perceptions concerned with health and wellbeing. Suitable candidate models that could be used to study this self-care dimension include Public Health Theory, Public Management Theory, Public Policy Theory and any existing Health in All Policy (HiAP) prescriptions, including directives for the built environment.
Model synthesis
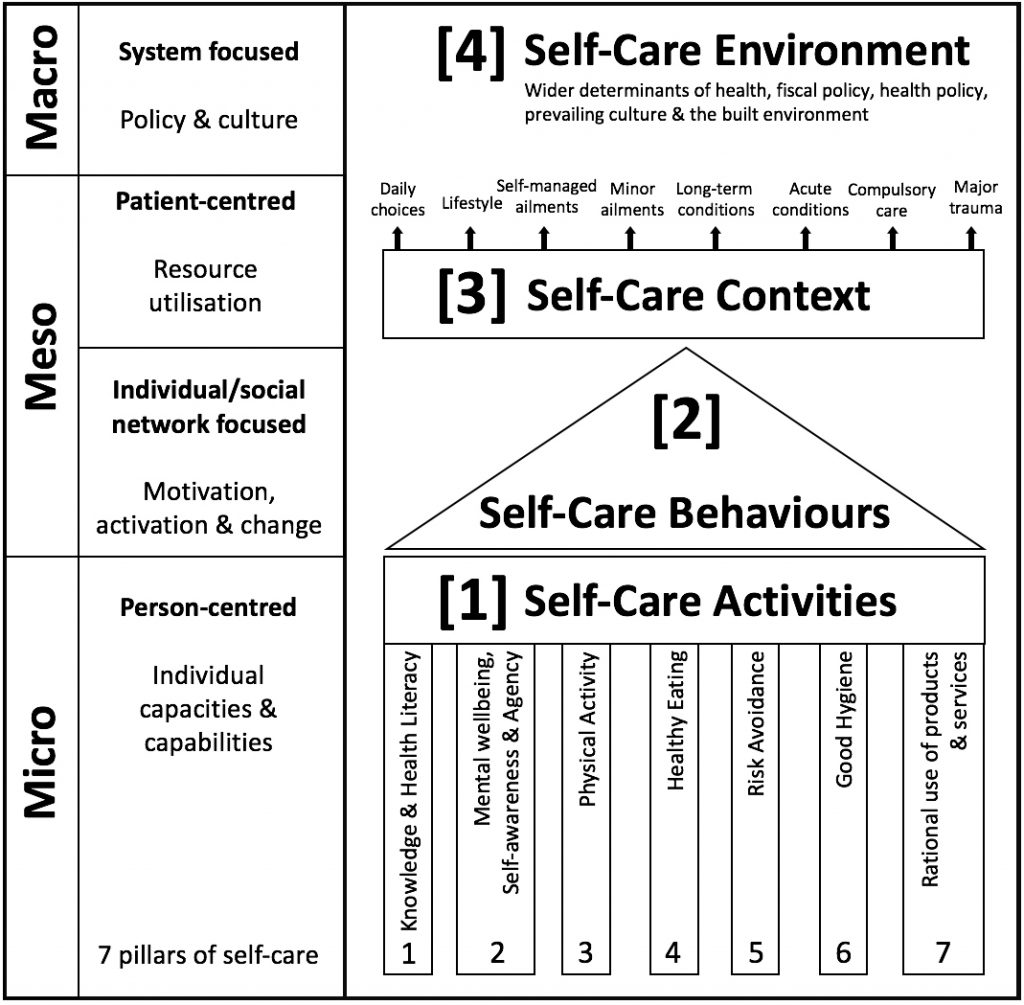
Figure 1 shows how the four cardinal dimensions of self-care can be juxtaposed on a matrix to illustrate the relationship between them. In this new conception, the Self-Care Matrix (SCM) is a synthesis of 32 existing models and frameworks which makes it possible to consider self-care in its totality (figure 1). The two left panes of the schema congruently describe the level of focus and the perspective relevant to each dimension of self-care. The schema also shows diagrammatically how self-care activities, behaviours and activation, and reliance on resources (i.e. dimensions 1-3) are sequentially connected, whereas the self-care environment (i.e. dimension 4) exerts an omnidirectional influence on all other three dimensions of self-care.
Figure 1: The Self-Care Matrix (SCM)
discussion
Self-care has been extensively defined and considered by various academic groups and conceptualised from many different perspectives (table 1). The lack of a unified conceptual framework that consolidates existing non-disease specific models and theories of self-care has been a significant barrier to the development of suitable self-care interventions in the contemporary setting. The strategic global development and adoption of a unified commonly-understood and widely accepted conceptual model of self-care is desirable and can benefit all stakeholders. It is also helpful to move towards understanding self-care as an applied field of research as opposed to framing the concept as a purist academic pursuit. To this end, we advance a comprehensive yet pragmatic model that supports the conceptualisation of self-care in its totality, and that can be used by all stakeholders.
The proposed Self-Care Matrix (SCM) signals a new point of departure for self-care thinking that could inform the development, commissioning and evaluation of self-care interventions. The proposed Self-Care Matrix (SCM) thus provides a new point of departure for self-care thinking that could inform the development, commissioning and evaluation of self-care interventions in the contemporary setting by describing various aspects that could be grouped into four interlinked dimensions.
Characterising the Self-Care Matrix
Our synthesis consolidated various perspectives gleaned from 32 existing models of self-care and considered emergent themes and domains which naturally grouped into four cardinal dimensions (table 2, figure 1). The SCM schema illustrates that each dimension operates at one of three independent levels (micro, meso and macro-level). Dimensions 1 and 2 of the Self-Care Matrix consider the individual from a person-centred perspective, while dimensions 3 and 4 frame the individual or a segment of the population from the medicalised patient perspective or a broader health system viewpoint.
Self-care involves a wide range of personal activities such as physical activity, healthy eating, good hygiene and the avoidance of risks such as tobacco and excessive alcohol consumption. Although it is recognised that these activities are inter-connected, they are often approached ‘vertically’ in public health programmes and tend to be considered as separate activities. The Self-Care Matrix thus provides a congruent system which covers all aspects of self-care, offers a logical connection between them, and creates a framework on which metrics can be based and developed. In this regard, SCM represents real-world conditions and provides a logical unifying framework for the individual – and all other stakeholders – to make sense of all the different self-care elements and their inter-connections.
Strength and limitations
A particular strength of SCM is that it emphasises the inter-relationship between the four dimensions of self-care. This can help stakeholders identify the various discrete elements that could impact self-care capacities and capabilities across a wide range of settings and scenarios (e.g. during urban and environmental planning, or the development of public health initiatives or person-centred self-care interventions). By way of illustration, many urban planners use Barton & Grant’s Settlement Health Map84 as their conceptual framework. The Health Map has been widely referenced by the WHO Healthy City programmes across the world, and is inspired by three sources: (1) theories of the social determinants of health, (2) principles of human ecology, and (3) an understanding of the disciplines of planning. The Health Map has clear antecedents in Hancock’s (1985) ‘mandala of health’85, which linked health to human ecosystems and discussions on the social determinants of health. Although the Settlement Health Map does not focus specifically on self-care, its concentric circles of ecosystem, environment, community and lifestyle are entirely consistent with the four dimensions of self-care expressed in the unifying Self-Care Matrix.
The principal limitation of our new conception is that the various models, theories, and frameworks of self-care used to synthesise the Self-Care Matrix did not result from a systematic review of the literature. However, our extensive pragmatic review identified the most widely used and accessible conceptions of self-care gleaned from academic and lay literature and with reference to statutory and non-governmental stakeholder groups concerned with the study and advocacy of self-care.
Integrating conceptual models with the evidence base
Because the Self-Care Matrix is a synthesis of existing theories and models, it is possible for stakeholders to use an evidence-based approach to inform the development of suitable self-care interventions for application across a wide range of settings. For example, SCM illustrates that the second dimension of behaviour, activation and change is linked to, but ultimately separate from the first dimension pertaining to self-care capacities, capabilities and activities. This delineation makes it possible to integrate the evidence base for behaviour change in a way that fosters the development of suitable self-care interventions through the application of knowledge from a broad range of behaviour change theories31,32,36,44,48,86. Interventions at this level may be developed that activate any number of pillars of self-care represented in the first dimension, whilst for example using incentivisation and gamification techniques to ensure traction and lead to sustained behaviour change in individuals represented in the second dimension.
Equally, the integration of the evidence base for the Self-Care Continuum54 represented by the third dimension in SCM can be supported through a detailed analysis of case finding, risk stratification and population segmentation. This could help make the economic case for the development and funding of coherent self-care initiatives aimed at reducing reliance on resources56, and the funding of social prescribing initiatives and workplace health promotion programmes that seek to promote the routine adoption of healthy lifestyle habits and health seeking behaviours to improve overall health and wellbeing.
Elucidating the relationship between the wider or external environment and how this can impact self-care activities and behaviours in a segment of society can help drive fiscal and public health policy prescriptions that could refocus health systems towards a Health in All Policy (HiAP) approach87. For example, the WHO final report of the Commission on Social Determinants of Health concluded that ‘social injustice is killing people on a grand scale’88, and identified key commonalities between primary health care and the social determinants of health paradigms. This places a central focus on health equity, which is relevant in all countries and contexts, regardless of income level, and considers health as more than the absence of disease89. This evidence base can be used to develop programmes which promote multi-sectoral action and the step-wise adoption of progressive HiAP and other self-care ‘best-buys’ and policy prescriptions.
The Self-Care Matrix is therefore a suitable tool that could be used to model the impact that an intervention could have on the various inter-related dimensions of self-care. To exemplify, the schema shows that an intervention that causes a change in self-care activities (Dimension 1) would not necessarily precipitate a change in an individual’s reliance on resources (Dimension 3) without the mediation of factors concerned with activation and the sustained adoption of a desirable lifestyle habits (Dimension 2). The schema also suggests that a change in the external environment (Dimension 4) could exert a powerful and omnidirectional influence on all other three dimensions of self-care. This analysis highlights the importance of resource mobilisation and policy development work to promote a progressive commissioning landscape which encourages the piloting of suitable evidence-based self-care interventions in the educational, applied care or community care settings.
Implications for policy makers and researchers
The emergence of long-term NCDs as a major health issue around the world has put the spotlight on self-care90. Through self-care, people can delay or prevent many chronic diseases such as coronary heart disease, strokes, diabetes and cancers, in which an unhealthy lifestyle is well established as a key causative agent91. Many countries have incorporated aspects of self-care into policies through innovative and notable practices92. However, all countries are a long way from implementing robust and meaningful policy prescriptions designed to promote individual and population wide self-care capabilities, whilst shifting professional practices and reorienting healthcare systems towards a preventative ethos. The development of self-care as an academic subject and as a practical choice for policymakers and health professionals presents important opportunities for the development of sustainable policy prescriptions that support a coherent ‘cradle to grave’ approach to national and international self-care narratives.
SCM can thus be used as a suitable lens by which to evaluate self-care interventions by considering different components of self-care across four dimensions, and provides a common framework for the study and development of policy prescriptions for self-care for application in the real-world setting. Objective evaluation of self-care initiatives using the SCM approach could help foster a culture of evidence-based commissioning for self-care interventions in the health and wellbeing space.
Summary & Conclusion
The proposed Self-Care Matrix is a pragmatic and unifying framework that can be used to conceptualise the totality of self-care and its various interlinked dimensions. SCM can be used as a lens by which to view, identify, study and evaluate self-care elements in any health and wellbeing intervention, independent of the disease category or setting. The mid-level descriptions and the visual schema illustrating the inter-relationship between each of the four cardinal dimensions of self-care render this model widely applicable and easily accessible to a wide audience, including policymakers, commissioners of health and all other self-care stakeholders. The Self-Care Matrix signals a new point of departure for self-care thinking and can be used as a common ground between all stakeholders interested in advancing the study, practice, development, commissioning and evaluation of self-care initiatives in the contemporary setting.
Correspondence to: Dr Austen El-Osta, The Self-Care Academic Research Unit (SCARU). Department of Primary Care & Public Health, Imperial College London, 323 Reynolds Building, Charing Cross Hospital, London W6 8RF.
Acknowledgements: Ms Evelina Barbanti (SCARU Research Assistant), Dr Ahmed Alboksmaty (SCARU Research Assistant), Ms Mashael Almadi (SCARU Research Assistant), Ms Farah Masood (SCARU Research Assistant) & Dr Marize Bakhet (SCARU Research Fellow) provided support in data acquisition and analysis.
Contributors: All authors provided substantial contributions to the conception (AEO, DW, SG, RB, DM, AM, PS), design (AEO, PS), acquisition of the data (AEO, EB, AA, MA, FM, MB), and the analysis and interpretation of the pragmatic review (AEO, DW). AEO, DW and PS did the decision making of the framework construction. AEO took the lead in planning the study with support from the co-authors and carried out the data analysis with support from AA, EB, DW and PS. AEO is the guarantor.
Funding: This article presents independent research in part funded by the National Institute for Health Research (NIHR) under the Collaborations for Leadership in Applied Health Research and Care (CLAHRC) programme for North West London. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
References
- Healthy Living Is the Best Revenge: Findings From the European Prospective Investigation Into Cancer and Nutrition–Potsdam StudyHealthy Living and Chronic Diseases. JAMA Internal Medicine. 2009;169(15):1355-62.
- Loef M, Walach H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Preventive Medicine. 2012;55(3):163-70.
- Dianne M. An Examination of the Self-Care Concept Uncovers a New Direction for Healthcare Reform. Nursing Leadership. 2003;16(4):48-65.
- Stearns SC, Bernard SL, Fasick SB, Schwartz R, Konrad TR, Ory MG, et al. The economic implications of self-care: the effect of lifestyle, functional adaptations, and medical self-care among a national sample of Medicare beneficiaries. American journal of public health. 2000;90(10):1608-12.
- Reilly CM, Butler J, Culler SD, Gary RA, Higgins M, Schindler P, et al. An economic evaluation of a self-care intervention in persons with heart failure and diabetes. Journal of cardiac failure. 2015;21(9):730-7.
- Company EPPCI. Self-Care Reduces Costs and Improves Health – The Evidence. 2010(1):1-16.
- Godfrey CM, Harrison MB, Lysaght R, Lamb M, Graham ID, Oakley P. Care of self – care by other – care of other: the meaning of self-care from research, practice, policy and industry perspectives. Int J Evid Based Healthc. 2011;9(1):3-24.
- Omisakin FD, Ncama B. Self, self-care and self-management concepts: Implications for self-management education. Educational Research. 2011;2(12):1733-7.
- Carlson B, Riegel B, Moser DK. Self-care abilities of patients with heart failure. Heart Lung [Internet]. 2001 Sep-Oct; 30(5):[351-9 pp.].
- Sharoni SKA, Abdul Rahman H, Minhat HS, Shariff Ghazali S, Azman Ong MH. A self-efficacy education programme on foot self-care behaviour among older patients with diabetes in a public long-term care institution, Malaysia: a Quasi-experimental Pilot Study. BMJ Open. 2017;7(6):1-10.
- Russell EM, Iljon-Foreman EL. Self-Care in Illness: a Review. Family Practice. 1985;2(2):108-21.
- 12. Levin LS, Idler EL. Self-care in health. Annual Review of Public Health. 1983;4(1):181-201.
- Godfrey CM. Self-care: a clarification of meaning and examination of supportive strategies: Queen’s University Kingston, Ontario, Canada; 2010.
- Matarese M, Lommi M, De Marinis MG, Riegel B. A Systematic Review and Integration of Concept Analyses of Self-Care and Related Concepts. J Nurs Scholarsh. 2018;50(3):296-305.
- Franek J. Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ont Health Technol Assess Ser. 2013;13(9):1-60.
- Balduino AdFA, Mantovani MdF, Lacerda MR, Meier MJ. Análise conceitual de autogestão do indivíduo hipertenso. Revista Gaúcha de Enfermagem. 2013;34:37-44.
- Hlatky MA, Boineau RE, Higginbotham MB, Lee KL, Mark DB, Califf RM, et al. A brief self-administered questionnaire to determine functional capacity (The Duke Activity Status Index). American Journal of Cardiology. 1989;64(10):651-4.
- Richard AA. Psychometric Testing of the Sidani and Doran Therapeutic Self-Care Scale in a Home Health Care Population. Journal of nursing measurement. 2016;24(1):92-107.
- Sidani S, Doran DI. Development and Validation of a Self-Care Ability Measure. CJNR. 2014;46(1):11-25.
- Hibbard JH, Mahoney ER, Stock R, Tusler M. Do Increases in Patient Activation Result in Improved Self-Management Behaviors? Health Services Research. 2007;42(4):1443-63.
- Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and Testing of a Short Form of the Patient Activation Measure. Health Services Research. 2005;40(6):1918-30.
- Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the Patient Activation Measure (PAM): Conceptualizing and Measuring Activation in Patients and Consumers. Health Services Research. 2004;39(4):1005-26.
- Dean K, Holst E, Kreiner S, Schoenborn C, Wilson R. Measurement issues in research on social support and health. J Epidemiol Community Health. 1994;48(2):201-6.
- Brenner MH, Curbow B, Legro MW. The Proximal-Distal Continuum of Multiple Health Outcome Measures: The Case of Cataract Surgery. Medical Care. 1995;33(4):AS236-AS44.
- Singh-Manoux A, Clarke P, Marmot M. Multiple measures of socio-economic position and psychosocial health: proximal and distal measures. International journal of epidemiology [Internet]. 2002; 31(6):[1192-9 pp.].
- Gantz SB. Self-care: Perspectives from six disciplines Holistic Nurse Practice 1990;4(2):1-12.
- Cameron J, Worrall-Carter L, Driscoll A, Stewart S. Measuring Self-care in Chronic Heart Failure: A Review of the Psychometric Properties of Clinical Instruments. Journal of Cardiovascular Nursing. 2009;24(6):E10-E22.
- Matarese M, Lommi M, De Marinis MG. Systematic review of measurement properties of self-reported instruments for evaluating self-care in adults. Journal of Advanced Nursing. 2017;73(6):1272-87.
- Richard M. Ryan HP, Edward L. Deci, and Geoffrey C. Williams. Facilitating health behaviour change and its maintenance: Interventions based on Self-Determination Theory. The European Health Psychologist [Internet]. 2008 12 April 2019; 10:[2-5 pp.]. Available from: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.460.1417&rep=rep1&type=pdf.
- Davis R, Campbell R, Hildon Z, Hobbs L, Michie S. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev. 2015;9(3):323-44.
- Bandura A. Social Cognitive Theory. In: Van Lange PAM, Kruglanski AW, Higgins ET, editors. Handbook of social psychological theories. 1. London: SAGE Publications; 2012. p. 349-73.
- Chapman-Novakofski K, Karduck J. Improvement in knowledge, social cognitive theory variables, and movement through stages of change after a community-based diabetes education program. Journal of the American Dietetic Association. 2005;105(10):1613-6.
- Schunk DH, Usher EL. Social Cognitive Theory. In: Harris KR, Graham S, Urdan TC, editors. APA Educational Psychology Handbook. 1: American Psychological Association; 2012. p. 101-23.
- Schwarzer R, Luszczynska A. Social cognitive theory. Predicting health behaviour. 2005;2:127-69.
- Becker G, Gates RJ, Newsom E. Self-Care Among Chronically Ill African Americans: Culture, Health Disparities, and Health Insurance Status. American Journal of Public Health. 2004;94(12):2066-73.
- Becker MH. The health belief model and personal health behavior. Thorofare, NJ: Slack; 1974. 154 p.
- Janz NK, Becker MH. The Health Belief Model: A Decade Later. Health Education Quarterly. 1984;11(1):1-47.
- Maiman LA, Becker MH. The health belief model: Origins and correlates in psychological theory. Health Education Monographs. 1974;2(4):336-53.
- Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health education quarterly. 1988;15(2):175-83.
- Fishbein M, Ajzen I. Predicting and changing behavior: The reasoned action approach. Mahwah, NJ: Lawrence Erlbaum Associates, Inc., Publishers; 2007. 328 p.
- Madden TJ, Ellen PS, Ajzen I. A Comparison of the Theory of Planned Behavior and the Theory of Reasoned Action. Personality and Social Psychology Bulletin. 1992;18(1):3-9.
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991;50(2):179-211.
- Fisher W, Fisher J, Harman J. The Information-Motivation-Behavioral Skills Model: A General Social Psychological Approach to Understanding and Promoting Health Behavior. In: Suls J, Wallston KA, editors. Social Psychological Foundations of Health and Illness2003. p. 82-106.
- Prochaska JO, Velicer WF. The Transtheoretical Model of Health Behavior Change. American Journal of Health Promotion. 1997;12(1):38-48.
- Ryan P. Integrated Theory of Health Behavior Change: Background and Intervention Development. Clinical Nurse Specialist [Internet]. 2009; 23(3):[161-72 pp.]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2778019/.
- Polly R, Marianne W, Nicole T, Michael B. Testing the Integrated Theory of Health Behaviour Change for postpartum weight management. Journal of Advanced Nursing. 2011;67(9):2047-59.
- Schwarzer R, Lippke S, Luszczynska A. Mechanisms of health behavior change in persons with chronic illness or disability: the Health Action Process Approach (HAPA). Rehabil Psychol. 2011;56(3):161-70.
- Michie S, van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science. 2011;6(1):42.
- International Self Care Foundation. The Seven Pillars of Self-Care Framework 2018 [2 April 2019]. Available from: https://isfglobal.org/seven-pillars-self-care-framework/.
- Self-Care Forum UK. The Self Care Continuum. What do we mean by self care and why is it good for people? 2010 [Available from: https://www.selfcareforum.org/about-us/what-do-we-mean-by-self-care-and-why-is-good-for-people/.
- Hartweg D. Dorothea Orem: Self-care deficit theory. Starika MR, editor: Sage Publications; 1991.
- Orem DE. A concept of self-care for the rehabilitation client. Rehabilitation nursing. 1985;10(3):33-6.
- Orem DE, Taylor SG, Renpenning KM. Nursing: Concepts of practice. 1995.
- Webber DE, Guo Z, Mann S. Self-care in health. We can define it, but should we also measure it? Self-Care Journal. 2013;4(5):101-6.
- Riegel B, Jaarsma T, Stromberg A. A middle-range theory of self-care of chronic illness. ANS Adv Nurs Sci. 2012;35(3):194-204.
- Roland M, Abel G. Reducing emergency admissions: are we on the right track?2012; 345:[1-6 pp.]. Available from: https://www.bmj.com/content/bmj/345/bmj.e6017.full.pdf.
- Horowitz LG. The Self-Care Motivation Model: Theory and Practice in Healthy Human Development. Journal of School Health. 1985;55(2):57-61.
- Haug MR, Wykle ML, Namazi KH. Self-care among older adults. Social Science & Medicine. 1989;29(2):171-83.
- Sorofman B, Tripp-Reimer T, Lauer GM, Martin ME. Symptom self-care. Holistic nursing practice. 1990;4(2):45-55.
- Simmons SJ. The Health-Promoting Self-Care System Model: directions for nursing research and practice. Journal of Advanced Nursing. 1990;15(10):1162-6.
- Leventhal H, Brissette I, Leventhal EA. The common-sense model of self-regulation of health and illness. In: Cameron L, Leventhal H, editors. The self-regulation of health and illness behaviour. Abingdon, Oxon: Routledge; 2003. p. 56-79.
- Leventhal H, Leventhal EA, Contrada RJ. Self-regulation, health, and behavior: A perceptual-cognitive approach. Psychology and Health. 1998;13(4):717-33.
- Makhubela BH. The Self-Care Model of Best Practice: Home Based Care. Africa Journal of Nursing and Midwifery. 2002;4(1):35-9.
- Leenerts MH, Teel CS, Pendleton MK. Building a model of self-care for health promotion in aging. J Nurs Scholarsh. 2002;34(4):355-61.
- Phoenix O. Self-Care Wheel 2013 [Available from: https://www.olgaphoenix.com/key-offerings/self-care-wheel/.
- Cammermeyer M. A growth model of self-care for neurologically impaired people. Journal of neurosurgical nursing. 1983;15(5):299-305.
- Connelly CE. Self-care and the chronically ill patient. The Nursing Clinics of North America. 1987;22(3):621-29.
- Raven M. A conceptual model for care in developmental disability services. The Australian journal of advanced nursing : a quarterly publication of the Royal Australian Nursing Federation. 1989;6(4):10-7.
- Lorig K. Chronic disease self-management – A model for tertiary prevention. Am Behav Sci. 1996;39(6):676-83.
- Backman K, Hentinen M. Model for the self-care of home-dwelling elderly. J Adv Nurs. 1999;30(3):564-72.
- Kennedy A, Rogers A, Bower P. Support for self care for patients with chronic disease. BMJ. 2007;335(7627):968-70.
- Rogers A, Vassilev I, Sanders C, Kirk S, Chew-Graham C, Kennedy A, et al. Social networks, work and network-based resources for the management of long-term conditions: a framework and study protocol for developing self-care support. Implementation Science [Internet]. 2011 2 April 2019 3120720]; 6:[56 p.]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21619695.
- Modi AC, Pai AL, Hommel KA, Hood KK, Cortina S, Hilliard ME, et al. Pediatric self-management: a framework for research, practice, and policy. Pediatrics. 2012;129(2):e473-85.
- Esperat MC, Flores D, McMurry L, Feng D, Song H, Billings L, et al. Transformacion Para Salud: a patient navigation model for chronic disease self-management. Online journal of issues in nursing. 2012;17(2):2.
- Bailey SC, Oramasionwu CU, Wolf MS. Rethinking adherence: a health literacy-informed model of medication self-management. J Health Commun. 2013;18 Suppl 1:20-30.
- Knight EP, Shea K. A patient-focused framework integrating self-management and informatics. J Nurs Scholarsh. 2014;46(2):91-7.
- Grey M, Schulman-Green D, Knafl K, Reynolds NR. A revised Self- and Family Management Framework. Nurs Outlook. 2015;63(2):162-70.
- Audulv A, Ghahari S, Kephart G, Warner G, Packer TL. The Taxonomy of Everyday Self-management Strategies (TEDSS): A framework derived from the literature and refined using empirical data2019 12 April 2019; 102:[367-75 pp.]. Available from: https://www.ncbi.nlm.nih.gov/pubmed/30197252.
- Forum SC. Self Care Forum: Helping people take care of themselves 2019 [Available from: https://www.selfcareforum.org/.
- Pines J, Selevan J, McStay F, George M, McClellan M. Kaiser Permanente – California: A Model for Integrated Care for the Ill and Injured.2015:[1-7 pp.]. Available from: https://docplayer.net/3251799-Kaiser-permanente-california-a-model-for-integrated-care-for-the-ill-and-injured.html.
- Riegel B, Dickson VV. A situation-specific theory of heart failure self-care. The Journal of cardiovascular nursing. 2008;23(3):190-6.
- Richard AA, Shea K. Delineation of self-care and associated concepts. J Nurs Scholarsh. 2011;43(3):255-64.
- PiSCE, editor Proposing policy actions on self-care at EU level (PiSCE – Pilot project on the promotion of self-care systems in the European Union). 2014-17; https://www.selfcare.nu/: PiSCE- EU.
- Barton H, Grant M. A health map for the local human habitat. Journal of the Royal Society for the Promotion of Health 2006;126(6):252-61.
- Hancock T. The mandala of health: a model of the human ecosystem. Family & community health. 1985;8(3):1-10.
- Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. . Reading, MA: Addison-Wesley; 1975.
- WHO. Health in All Policies: Framework for Country Action WHO. 2013.
- Rasanathan K. 10 years after the Commission on Social Determinants of Health: social injustice is still killing on a grand scale. The Lancet. 2018;392(10154):1176-7.
- Rasanathan K, Montesinos EV, Matheson D, Etienne C, Evans T. Primary health care and the social determinants of health: essential and complementary approaches for reducing inequities in health. J Epidemiol Community Health. 2011;65(8):656-60.
- Narasimhan M, de Iongh A, Askew I, Simpson PJ. It’s time to recognise self care as an integral component of health systems. BMJ. 2019;365:l1403.
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013-2020. Geneva, Switzerland: World Health Organisation; 2013.
- WHO. WHO Framework Convention on Tobacco Control. 2003.